

Abstract
The aim of allogeneic stem cell transplantation (SCT) is to combine tumor cytoreduction with optimal doses of chemoradiotherapy and to replace host with donor immunohematopoietic cells. Induction of host-vs.-graft tolerance by engraftment of donor stem cells, enables durable engraftment of donor lymphocytes, with subsequent induction of graft vs. leukemia effect (GVL) expected to eliminate all residual chemoradio-resistant malignant cells of host origin by alloreactive donor cells. Relapse shortly post SCT indicates tumor refractoriness and carries poor prognosis.
Multi-donor stem cell transplantation (MDT) is an innovative transplantation strategy aiming at both increasing the number of donor stem cells infused to the recipient to improve the chance of engraftment of at least one of the donors, thus avoiding the need for re-transplantation in case of rejection, while in parallel improving the displacement of residual host cells and GVL effect by stimulation of alloreactive donor T cells as bystander effect to the rejection of 1 donor by the other donor in order.
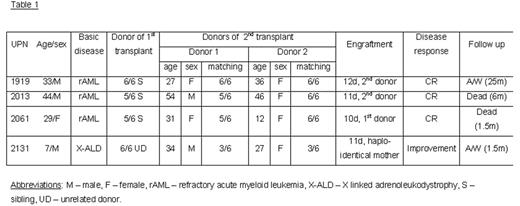
We describe 4 patients that were treated with MDT following early post allogeneic transplant relapse (n=3, resistant AML) or rejection (n=1). In order to reduce the risk for the patients, and with the assumption that MDT will stimulate anti host immune response leading to engraftment and GVL, we chose to combine transplantation from 2 donors (including the 1st donor in the patients transplanted due to relapse and both parents in the patient transplanted due rejection). The patients received a non myeloablative conditioning treatment. All patients engrafted (2 with the 2nd donor, 1 with 1st donor and 1 from his mismatched mother) with 100% donor chimera. Time to engraftment was short - median 11d (range 10–12). CR was achieved with the appearance of GVHD probably due to stimulation of donor vs. donor (and therefore against host alloantigens). No relapse was documented during follow up. Two of the recipients are currently alive with follow-up ranging 1.5–25m.
Conclusions: The use of MDT induced engraftment and GVL in patients with chemo-immuno-resistant leukemia. In view of the profound anti host activating effect of MDT, we plan to assess its therapeutic potential on engraftment facilitation when reduced intensity conditioning is used in patients in need for SCT lacking an HLA matched related or unrelated donor.
Disclosure: No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal