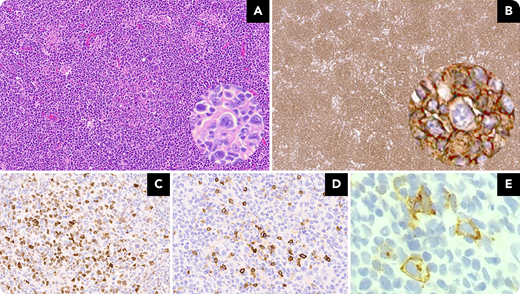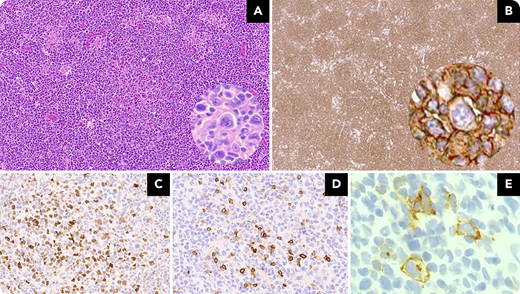
A 74-year-old man presented with recurrent respiratory infections without B symptoms, with mediastinal and supraclavicular lymphadenopathy on chest computed tomography. A fine-needle biopsy of a supraclavicular lymph node revealed distorted architecture with vaguely nodular growth, predominantly composed of medium-large cells with centroblastic morphology, rare centrocytes, and abundant mitotic activity (panel A; 10× objective, ×100 original magnification). Also identified were scattered, large, binucleated Reed-Sternberg–like and variant-like cells (panel A, inset; 40× objective, ×400 original magnification). The neoplastic population, including the Hodgkin-like cells, was CD20+ (panel B; 4× objective, ×40 original magnification; inset, 40× objective, ×400 original magnification); PAX5+, MUM1+, p53+, and bcl2+; weakly bcl6+ (panel C; 10× objective, ×100 original magnification); and CD10+ (panel D; 10× objective, ×100 original magnification), with >50% c-myc expression in the centroblastic cells. The Hodgkin-like cells were CD30+ (panel E; 40× objective, ×400 original magnification). Ki-67 showed a proliferative index of 60% to 70%; CD23 highlighted the dendritic meshwork. Flow cytometry revealed a CD19+/CD20+/CD5(partial) population with κ-chain restriction. Molecular testing showed 3 clinically significant variants: CREBBP, KMT2D/MLL2, and TNFAIP3. No abnormalities were detected in BCL2, and no translocations were identified. Reed-Sternberg–like cells have been described in cases of follicular lymphoma, independent of grade, and they have been shown to be clonally related to the follicular lymphoma cell population. The importance of these cells lies in the diagnostic challenge they create and possibly in providing early evidence of transformation.
A 74-year-old man presented with recurrent respiratory infections without B symptoms, with mediastinal and supraclavicular lymphadenopathy on chest computed tomography. A fine-needle biopsy of a supraclavicular lymph node revealed distorted architecture with vaguely nodular growth, predominantly composed of medium-large cells with centroblastic morphology, rare centrocytes, and abundant mitotic activity (panel A; 10× objective, ×100 original magnification). Also identified were scattered, large, binucleated Reed-Sternberg–like and variant-like cells (panel A, inset; 40× objective, ×400 original magnification). The neoplastic population, including the Hodgkin-like cells, was CD20+ (panel B; 4× objective, ×40 original magnification; inset, 40× objective, ×400 original magnification); PAX5+, MUM1+, p53+, and bcl2+; weakly bcl6+ (panel C; 10× objective, ×100 original magnification); and CD10+ (panel D; 10× objective, ×100 original magnification), with >50% c-myc expression in the centroblastic cells. The Hodgkin-like cells were CD30+ (panel E; 40× objective, ×400 original magnification). Ki-67 showed a proliferative index of 60% to 70%; CD23 highlighted the dendritic meshwork. Flow cytometry revealed a CD19+/CD20+/CD5(partial) population with κ-chain restriction. Molecular testing showed 3 clinically significant variants: CREBBP, KMT2D/MLL2, and TNFAIP3. No abnormalities were detected in BCL2, and no translocations were identified. Reed-Sternberg–like cells have been described in cases of follicular lymphoma, independent of grade, and they have been shown to be clonally related to the follicular lymphoma cell population. The importance of these cells lies in the diagnostic challenge they create and possibly in providing early evidence of transformation.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.