

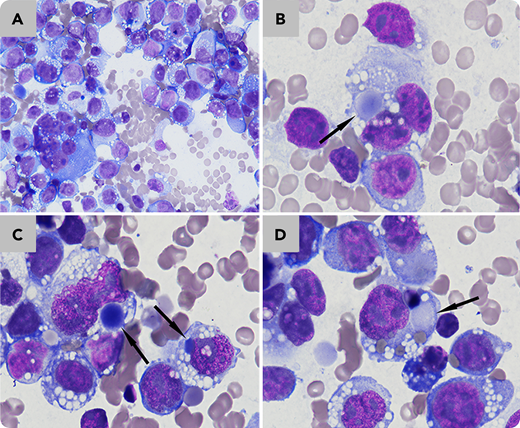
A 13-year-old boy with a history of left knee joint and back pain presented with severe discomfort, inguinal lymphadenopathy, thrombocytopenia, and anemia (white blood cell count 4.1 × 109/L, hemoglobin 9.4 g/dL, platelets 106 × 109/L). Magnetic resonance imaging revealed infiltrations in the extracranial soft tissue, mastoid, pleura, paralumbosacral soft tissue, testes, pelvic lymph nodes, and bone marrow. Peripheral blood film suggested normocytic anemia. Bone marrow aspirate analysis showed 78% uninucleated to binucleated to multinucleated large cells with basophilic cytoplasm and cytoplasmic vacuoles, sometimes adhesive and clustered (panel A; Wright-Giemsa stain, 40× objective; total magnification ×400); 5% of these cells contained paranuclear blue inclusions (panels B-D; Wright-Giemsa stain, 100× objective; total magnification ×1000). Needle biopsy of the patient’s swollen inguinal lymph nodes revealed rhabdomyosarcoma, with cells positive for vimentin, desmin, myogenin, and myoD1. The boy’s condition deteriorated rapidly, and he died on day 11 after admission.
Paranuclear blue inclusions are known to be a feature of lung small cell carcinoma and can also be observed in rhabdomyosarcoma or even non-Hodgkin lymphoma. However, they are not a common feature of rhabdomyosarcoma. Moreover, a definitive diagnosis of rhabdomyosarcoma requires tissue biopsy and immunohistochemical examinations.
A 13-year-old boy with a history of left knee joint and back pain presented with severe discomfort, inguinal lymphadenopathy, thrombocytopenia, and anemia (white blood cell count 4.1 × 109/L, hemoglobin 9.4 g/dL, platelets 106 × 109/L). Magnetic resonance imaging revealed infiltrations in the extracranial soft tissue, mastoid, pleura, paralumbosacral soft tissue, testes, pelvic lymph nodes, and bone marrow. Peripheral blood film suggested normocytic anemia. Bone marrow aspirate analysis showed 78% uninucleated to binucleated to multinucleated large cells with basophilic cytoplasm and cytoplasmic vacuoles, sometimes adhesive and clustered (panel A; Wright-Giemsa stain, 40× objective; total magnification ×400); 5% of these cells contained paranuclear blue inclusions (panels B-D; Wright-Giemsa stain, 100× objective; total magnification ×1000). Needle biopsy of the patient’s swollen inguinal lymph nodes revealed rhabdomyosarcoma, with cells positive for vimentin, desmin, myogenin, and myoD1. The boy’s condition deteriorated rapidly, and he died on day 11 after admission.
Paranuclear blue inclusions are known to be a feature of lung small cell carcinoma and can also be observed in rhabdomyosarcoma or even non-Hodgkin lymphoma. However, they are not a common feature of rhabdomyosarcoma. Moreover, a definitive diagnosis of rhabdomyosarcoma requires tissue biopsy and immunohistochemical examinations.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

