


Background: Patients (pts) with relapsed/refractory (R/R) Philadelphia chromosome-positive acute lymphoblastic leukemia (Ph+ ALL) have poor outcomes, and there is no clear standard of care. While the pan-BCR-ABL tyrosine kinase inhibitor (TKI) ponatinib is highly active in Ph+ ALL, single-agent responses are short-lived. Ph+ ALL is highly dependent on Bcl-2 for survival, suggesting a possible therapeutic role for venetoclax in this disease. Preclinical studies suggest that ponatinib and venetoclax result in synergistic anti-leukemia activity through inhibition of the Lck/Yes novel (LYN) tyrosine kinase by ponatinib and its downstream prevention of Mcl-1 upregulation (Leonard JT et al. Sci Trans Med 2016;8(354)). We therefore designed a phase I/II study to evaluate the safety and efficacy of the combination of ponatinib, venetoclax, and dexamethasone in pts with R/R Ph+ ALL.
Methods: Adults ≥18 years of age with R/R Ph+ ALL or chronic myeloid leukemia in lymphoid blast phase who had received at least 1 prior BCR-ABL TKI were eligible. For cycle 1, pts without recent ponatinib exposure (i.e. within 2 weeks) received a 7-day run-in of ponatinib monotherapy with ponatinib given at a dose of 45 mg daily on days 1-35, venetoclax daily on days 8-35 (up to 400mg in dose level 1; up to 800mg in dose level 2), and dexamethasone 40mg IV/PO daily on days 8-11. Pts with recent ponatinib exposure received all three agents beginning on day 1 of cycle 1. For cycles 2+, all pts received venetoclax 400-800mg daily on days 1-28, ponatinib daily on days 1-28, and dexamethasone 40mg IV/PO daily on days 1-4. The dose of ponatinib was adjusted according to the remission status, with pts who had not achieved CR/CRi receiving 45mg daily, those in CR/CRi but still with detectable BCR-ABL1 by PCR receiving 30mg daily, and those in complete molecular response (CMR) receiving 15 mg daily. Each cycle was 28 days. All pts received 8 administrations of intrathecal chemotherapy. Up to 8 doses of rituximab were added for CD20+ disease. The primary safety objective was to determine the maximum tolerated dose (MTD) of venetoclax in combination with ponatinib and dexamethasone, and the primary efficacy objective was to determine the CR/CRi rate of the regimen.
Results: To date, 8 pts have been enrolled, and 6 pts have been treated and are evaluable for safety and efficacy. Three pts received venetoclax 400mg daily, and 3 pts received venetoclax 800mg daily. The median number of courses given was 3 (range, 1-8). No dose-limiting toxicities have been observed, and the MTD has not yet been reached. Non-hematologic grade 3-4 adverse events included: ALT/AST elevation and febrile neutropenia in 2 pts each, and GI hemorrhage, altered mental status, lower extremity weakness, and infection in 1 pt each. There were no early deaths.
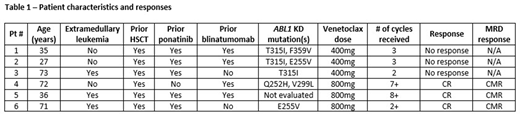
The characteristics of the treated pts and their responses are shown in Table 1. The median age was 53 years (range, 27-73 years). All pts had received prior allogeneic hematopoietic stem cell transplant. The median number of prior therapies was 3.5 (range, 2-4) and median number of prior TKIs was 2 (range, 1-3). Five pts (83%) had received prior ponatinib and 4 (67%) had received blinatumomab. Three pts (50%) had extramedullary disease, and 3 of 5 pts (60%) who underwent ABL1 kinase domain testing had a detectable T315I mutation.
Overall, 3 pts (50%) achieved CR. Notably, all pts who achieved CR received the 800mg daily dose of venetoclax. Two responses were in pts who had received prior ponatinib, and 2 were in pts who had received prior blinatumomab. One pt who received venetoclax 400mg daily had bone marrow blast decrease from 94% to 6% after cycle 1 along with full neutrophil recovery and platelet recovery to 97 x 109/L (though not meeting formal criteria for partial remission). Among the 3 pts who achieved CR, all achieved CMR and remain on study. At last follow-up, all responding pts remain in ongoing CMR with remission durations of 1 month, 5 months, and 8 months, respectively. With a median duration of follow-up of 8.6 months, the median OS has not been reached, and the estimated 9-month OS rate is 60%.
Conclusions: The chemotherapy-free, oral combination of ponatinib, venetoclax and dexamethasone appears safe and has promising early efficacy in this heavily pretreated population of pts with R/R Ph+ ALL, with all 3 pts who received venetoclax 800mg daily achieving CMR. The MTD has not yet been reached, and the study continues to accrue.
Short:AstraZeneca: Consultancy; Takeda Oncology: Consultancy, Honoraria, Research Funding; Amgen: Honoraria; Astellas: Research Funding. Konopleva:Reata Pharmaceutical Inc.;: Patents & Royalties: patents and royalties with patent US 7,795,305 B2 on CDDO-compounds and combination therapies, licensed to Reata Pharmaceutical; Forty-Seven: Consultancy, Research Funding; Ablynx: Research Funding; Stemline Therapeutics: Consultancy, Research Funding; Sanofi: Research Funding; Calithera: Research Funding; Rafael Pharmaceutical: Research Funding; Ascentage: Research Funding; Agios: Research Funding; AstraZeneca: Research Funding; F. Hoffmann La-Roche: Consultancy, Research Funding; Genentech: Consultancy, Research Funding; Cellectis: Research Funding; AbbVie: Consultancy, Research Funding; Kisoji: Consultancy; Eli Lilly: Research Funding; Amgen: Consultancy. Jabbour:Genentech: Other: Advisory role, Research Funding; AbbVie: Other: Advisory role, Research Funding; Adaptive Biotechnologies: Other: Advisory role, Research Funding; Takeda: Other: Advisory role, Research Funding; Pfizer: Other: Advisory role, Research Funding; BMS: Other: Advisory role, Research Funding; Amgen: Other: Advisory role, Research Funding. Kadia:Pfizer: Honoraria, Research Funding; Astra Zeneca: Research Funding; Pulmotec: Research Funding; Abbvie: Honoraria, Research Funding; Cyclacel: Research Funding; Ascentage: Research Funding; Incyte: Research Funding; BMS: Honoraria, Research Funding; Amgen: Research Funding; Celgene: Research Funding; Astellas: Research Funding; Genentech: Honoraria, Research Funding; JAZZ: Honoraria, Research Funding; Cellenkos: Research Funding; Novartis: Honoraria. Daver:Daiichi Sankyo: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Gilead: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Amgen: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Trovagene: Research Funding; Fate Therapeutics: Research Funding; ImmunoGen: Research Funding; Novartis: Consultancy, Membership on an entity's Board of Directors or advisory committees; Celgene: Consultancy, Membership on an entity's Board of Directors or advisory committees; Jazz: Consultancy, Membership on an entity's Board of Directors or advisory committees; Trillium: Consultancy, Membership on an entity's Board of Directors or advisory committees; Syndax: Consultancy, Membership on an entity's Board of Directors or advisory committees; Amgen: Consultancy, Membership on an entity's Board of Directors or advisory committees; KITE: Consultancy, Membership on an entity's Board of Directors or advisory committees; Agios: Consultancy, Membership on an entity's Board of Directors or advisory committees; Bristol-Myers Squibb: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Pfizer: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Karyopharm: Research Funding; Servier: Research Funding; Genentech: Research Funding; AbbVie: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Astellas: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Novimmune: Research Funding. Jain:Genentech: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Pharmacyclics: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; BMS: Research Funding; AstraZeneca: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Pfizer: Research Funding; ADC Therapeutics: Research Funding; Incyte: Research Funding; Servier: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Cellectis: Research Funding; Verastem: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Adaptive Biotechnologies: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Precision Bioscienes: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Fate Therapeutics: Research Funding; Aprea Therapeutics: Research Funding; Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees; TG Therapeutics: Honoraria, Membership on an entity's Board of Directors or advisory committees; BeiGene: Honoraria, Membership on an entity's Board of Directors or advisory committees. Ravandi:Amgen: Consultancy, Honoraria, Research Funding; AstraZeneca: Consultancy, Honoraria; Celgene: Consultancy, Honoraria; BMS: Consultancy, Honoraria, Research Funding; Abbvie: Consultancy, Honoraria, Research Funding; Xencor: Consultancy, Honoraria, Research Funding; Jazz Pharmaceuticals: Consultancy, Honoraria, Research Funding; Astellas: Consultancy, Honoraria, Research Funding; Orsenix: Consultancy, Honoraria, Research Funding; Macrogenics: Research Funding.
This icon denotes a clinically relevant abstract

