

Introduction
Chronic expansion of large granular lymphocytes (LGL) has been reported after classical matched allogeneic hematopoietic stem cell transplantation (SCT) with bone marrow, peripheral (PB) or cord blood (CB) as source of graft. This proliferation is indolent and carries a favorable prognosis. Little is known of the incidence and features of LGL expansions in haplo-SCT with post-transplant cyclophosphamide (PTCy), where the impact of the duration of lymphopenia is also ill-documented.
Patients & methods
This study included 85 adult patients (pts) who received a haplo-SCT between 11/2013 and 03/2019 for hematological diseases. The 3 conditioning regimen used were i) Baltimore (n=28, 11/2013-05/2017) i.e. fludarabine 30 mg/m²/day (d), d -6 to -2, cyclophosphamide 14.5 mg/kg d -6, low dose total body irradiation (LDTBI) 2 Grays d-1, ii) Clo-Baltimore (n=28, 03/2014-04/2017), i.e. Clofarabine 30 mg/m²/d, d -6 to -2, cyclophosphamide 14.5 mg/kg d -6, LDTBI 2 Grays d -1, iii) CloB2A1 (n=29, 05/2017-03/2019) with Clofarabine 30 mg/m²/d,d -6 to -2, busulfan 3,4 mg/kg d -3 and -2, ATG 2,5 mg/kg d-1. All pts received mobilized PB as SC source on d 0 and PTCY 50 mg/kg/d on d +3 and +4 with cyclosporine and mycophenolate mofetyl as graft versus host disease (GVHD) prophylaxis. All pts provided informed consent for data collection.
The duration of lymphopenia (<1.5x109/L) as well as occurrence, duration and immunophenotype of LGL expansion (>4x109/L) were recorded. The patients with primary graft failure (n=6) or dead before 3 months (mo) post-SCT were excluded (n=7). Engraftment was monitored by qPCR on PB cells and sorted CD3+ T-cells. TCR-γ/β gene rearrangements of CD3+ collected during sustained lymphocytosis were assessed with the Biomed-2 PCR method (n=7). Data were analyzed considering viral reactivation episodes (CMV, EBV, HHV6 or BK virus), acute or chronic GVHD, relapse and survival.
Results
The study included 72 adults treated with haplo-SCT (43 males, median age: 59 yo (24-71)) with a median follow-up of 31 mo for alive patients. Most pts had a myeloid disease (64%) and 57% were in complete remission at the time of haplo-SCT. The median duration of lymphopenia was 6 mo (1-49), significantly shorter in pts with a CloB2A1 conditioning (151 d vs. Baltimore 293 d vs. Clo-Baltimore 387 d, p=0.003) or with CMV reactivation (138 d vs 361 d, p<0.0001).
Brisk LGL expansion was characterized morphologically in 10 pts (14%), of donor origin in the 9 pts tested. It occurred at a median of 5 mo (2-8), whatever the GVHD prophylaxis. These pts had a shorter duration of lymphopenia (4 vs 10 mo, p=0.0002). The median duration of LGL expansion was 6 mo (0.1-22) with a median lymphocyte count of 5.8x109/L (4.3-19.4). Immunophenotyping disclosed expansions of NK-cells (n=2), CD8+ CD4- T-cells (n=6) or CD4- CD8- TCR gd T-cells (n=2). They were oligoclonal (n=4) or monoclonal (n=3). A recipient CMV+ status was strongly associated with the onset of LGL expansion (89% vs 20%, p=0.0001), and with CMV reactivation (35% vs 4%, p=0.001) but not with that of other viruses. Grade 2-4 acute and chronic GVHD were not correlated with LGL expansion.
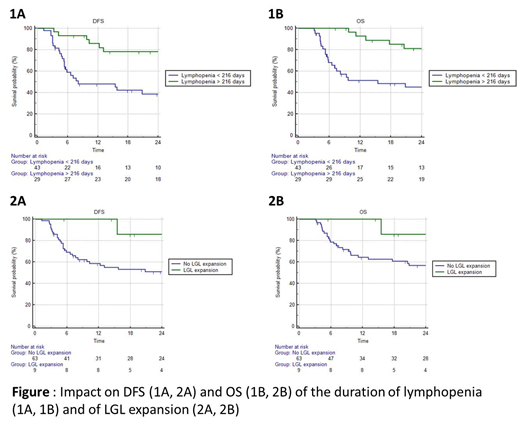
ROC curve analyses identified that pts with more than 216 d of lymphopenia (AUC=0.83, p<0.001) had a better 2y disease-free survival (DFS) (77% vs 38%, p=0.0008) and 2y overall survival (OS) (81% vs 45%, p =0.0006) (Fig. 1). LGL expansion was associated with a significantly lower incidence of relapse (10% vs 50%, p=0.03), better 2y-DFS (86% vs. 51%, p=0.05) and a trend towards a better 2y-OS (86% vs. 54%, p=0.1) (Fig. 2). Only 1 of these pts has relapsed and died of transplant-related mortality. Neither the recipient's CMV status nor CMV reactivation influenced DFS or OS. Multivariate analysis showed that the disease risk index score (Armand 2014), lymphopenia (>216 days) and LGL expansion, but not age (> 60yo), were independently associated with a better DFS and OS (p<0.0001).
Conclusion
A shorter duration of lymphopenia after haplo-SCT confers unexpectedly shorter survivals, suggesting the expansion of non-allo-reactive T-cells with a reduced graft versus leukemia effect. LGL expansion (14%) is not a rare event after haplo-SCT, mainly involves CD8+ T-cells, occurs preferably in CMV+ recipients or in pts with CMV reactivation. It is associated with a favorable outcome, similar to that observed in matched and CB SCT.
Peterlin:AbbVie Inc: Consultancy; Jazz Pharma: Consultancy; Daiichi-Sankyo: Consultancy; Astellas: Consultancy. Le Gouill:Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel support; Roche-Genentech: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel support. Chevallier:Incyte: Consultancy, Honoraria; Daiichi Sankyo: Honoraria; Jazz Pharmaceuticals: Honoraria.

