

A 35-year-old man presented with weakness, dyspnea, fevers, and mucosal bleeding. Complete blood count showed normocytic anemia (5.0 g/dL), severe thrombocytopenia (6000/mm3), and circulating blasts. Bone marrow core biopsy was hypercellular, with 42% blasts and 14% eosinophils enumerated on the aspirate with a marrow flow cytometry showing CD34, CD117, and myeloperoxidase positive blasts, consistent with the diagnosis of acute myeloid leukemia (AML).
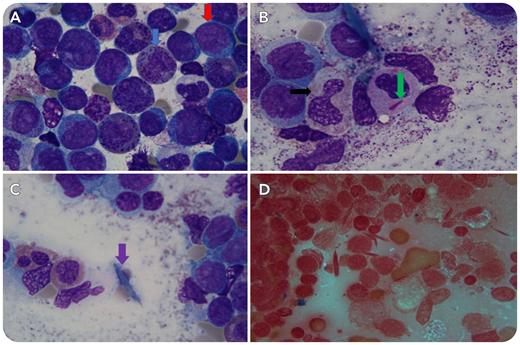
On examination of the aspirate (panels A-C, Wright-Giemsa stain, original magnification ×1000; panel D, Prussian blue iron stained, original magnification ×1000), in addition to the large population of blasts (panel A, red arrow, original magnification ×1000), numerous mature and immature eosinophils were seen. Some eosinophils appeared dysplastic (panel B, black arrow, original magnification ×1000), some demonstrated dark purple proeosinophilic granules (panel A, blue arrow, original magnification ×1000), and rare neutrophils had cytoplasmic Auer rods (panel B, green arrow, original magnification ×1000). Additionally, scattered pale nonpolarizing crystals were seen extracellularly (panel C, purple arrow, original magnification ×1000). A Prussian blue iron stained aspirate slide (panel D, original magnification ×1000) highlighted numerous crystals. Nuclear-Fast Red stain, a background stain used with the iron stain, highlighted the crystals, whereas iron stains blue. With the presence of abnormal eosinophils in the setting of AML, these nonpolarizing crystals are most consistent with Charcot-Leyden crystals. Cytogenetics showed a complex karyotype, including inv(16). This inv(16) AML demonstrated eosinophilia with Charcot-Leyden crystals. Of note, adequately prepared iron-stained aspirate slides highlight Charcot-Leyden crystals not seen well on Wright-Giemsa staining.
A 35-year-old man presented with weakness, dyspnea, fevers, and mucosal bleeding. Complete blood count showed normocytic anemia (5.0 g/dL), severe thrombocytopenia (6000/mm3), and circulating blasts. Bone marrow core biopsy was hypercellular, with 42% blasts and 14% eosinophils enumerated on the aspirate with a marrow flow cytometry showing CD34, CD117, and myeloperoxidase positive blasts, consistent with the diagnosis of acute myeloid leukemia (AML).
On examination of the aspirate (panels A-C, Wright-Giemsa stain, original magnification ×1000; panel D, Prussian blue iron stained, original magnification ×1000), in addition to the large population of blasts (panel A, red arrow, original magnification ×1000), numerous mature and immature eosinophils were seen. Some eosinophils appeared dysplastic (panel B, black arrow, original magnification ×1000), some demonstrated dark purple proeosinophilic granules (panel A, blue arrow, original magnification ×1000), and rare neutrophils had cytoplasmic Auer rods (panel B, green arrow, original magnification ×1000). Additionally, scattered pale nonpolarizing crystals were seen extracellularly (panel C, purple arrow, original magnification ×1000). A Prussian blue iron stained aspirate slide (panel D, original magnification ×1000) highlighted numerous crystals. Nuclear-Fast Red stain, a background stain used with the iron stain, highlighted the crystals, whereas iron stains blue. With the presence of abnormal eosinophils in the setting of AML, these nonpolarizing crystals are most consistent with Charcot-Leyden crystals. Cytogenetics showed a complex karyotype, including inv(16). This inv(16) AML demonstrated eosinophilia with Charcot-Leyden crystals. Of note, adequately prepared iron-stained aspirate slides highlight Charcot-Leyden crystals not seen well on Wright-Giemsa staining.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

