

Abstract
Abstract 2562
Massive parallel sequencing technology has elucidated the mechanism of molecular clonal evolution in relapsed AML patients (pts). However incidence and prognostic relevance of clonal evolution in real clinical setting is unknown. The aims of the current analysis are to: 1) evaluate incidence of clonal evolution both at cytogenetic and molecular level in relapsed and refractory AML pts using readily available molecular mutation panels, and 2) evaluate prognostic impact of both cytogenetic and molecular clonal evolution in such pts.
We analyzed 87 pts with AML who relapsed after induction therapy or who were refractory to induction and received 1st salvage therapies. If available, results of conventional cytogenetic study and molecular mutation panel including FLT3 (D835 and ITD), KRAS, NRAS, IDH1/2, NPM1, CEBPA, JAK2 and C-KIT were compared between the initial diagnosis and at time of relapse or at disease progression. Cytogenetic clonal evolution (CyE) was defined as acquisition of new cytogenetic abnormalities. Molecular clonal evolution (ME) was defined when there was acquisition of new genetic mutation not present at initial diagnosis.
Median age of the analyzed group was 61years (range: 17–82); 37 (43%) pts were female. Sixty three (72%) pts had de novo AML and 24 (28%) had secondary AML (evolved from MDS). Nineteen (22%) pts had prior cancer history and had exposure to chemo and/or radiation therapy (ie. therapy related AML). Fifty three (61%) pts received conventional high dose cytarabine-based regimen for the induction, 17 (19%) received clofarabine-based, 6 (7%) received sapacitabine, and 3 (3%) received low dose cytarabine-based regimen. Thirty six (41%) pts achieved complete remission (CR) after induction with median 1st CR duration of 5.7 months (range: 1.0–16.4), while 51 (59%) pts were refractory to it.
Baseline cytogenetics were diploid in 38 (44%) pts. Del 5q/−5was identified in 14 (16%) pts and del 7q/−7 was found in 21 (24%) pts. Complex cytogenetic abnormalities were seen in 26 (29%) pts. CyE was identified in 38 (44%) pts, of which 16 were seen at time of relapse and 22 at disease progression in refractory pts. Fifteen cases evolved from diploid and 23 developed from abnormal karyotype. Original founding cytogenetic abnormalities were persistently observed after evolution in all cases. Acquisition of trisomy 8 occurred in 6 (16%) pts, del7q/−7 in 4 (11%) and del5q/−5 in 2 (2%). Statistical association was not identified between development of CyE and other covariates (de novo vs. secondary AML, baseline cytogenetics, baseline molecular mutations, sex, therapy-related, baseline WBC, Hb, Plt, ME and presence of each molecular mutation).
Initial molecular mutation was detected in 40 (46%) pts. FLT3 D835 mutation was detected in 4 (5%), FLT3-ITD in 14 (16%), NPM1 in 10 (12%), NRAS in 13 (15%), CEBPA in 5 (6%), IDH1 in 4 (5%), IDH2 in 5 (6%), c-KIT in 1 (1%) pts, respectively. ME was identified in 12 (14%) pts of which 3 were seen at time of relapse and 9 were seen at time of disease progression in refractory pts. Among the observed ME, acquisition of FLT3-D835 mutation was seen in 6 patients (4 in pts originally with ITD mutation), FLT3-ITD acquisition in 3, NRAS acquisition in 2 and KRAS acquisition in 1 pts, respectively. Statistical association was not identified between development of ME and other covariates that were tested for CyE.
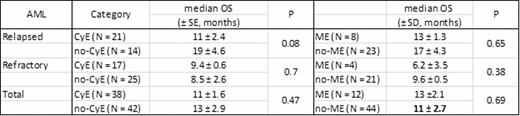
During the median follow up duration of 8.4 months (range 1–25), 47 (54%) pts were dead. Median overall survival (OS) of the total analyzed group was 10 months. Having CyE or ME did not affect OS (P = 0.47 and P = 0.70). Among the pts who relapsed after an initial CR (N= 36), a trend to worse OS was observed in pts with CyE (P = 0.08) but having ME did not affect OS (P = 0.65). In refractory AML pts (N= 51), having CyE or ME did not affect OS (P = 0.70 and P = 0.38) (Table 1).
Approximately 44% and 14% of pts with relapsed/refractory AML experience CyE or ME, respectively, either at time of relapse or progression. Neither CyE nor ME have significant prognostic relevance but an unfavorable trend was observed in relapsed AML pts with CyE at relapse. Larger series are needed to confirm a possible association. Sequential cytogenetic and molecular mutation analysis may be important in relapsed/refractory AML pts upon disease progression especially molecularly targeted agents are considered.
OS in relapsed/refractory AML +/− CyE or ME.
No relevant conflicts of interest to declare.
This icon denotes a clinically relevant abstract

