

Key Points
Ixazomib, cyclophosphamide, and dexamethasone combination achieved hematologic response in 63% of newly diagnosed AL amyloidosis patients.
The regimen is characterized with a favorable adverse event profile and should be explored in other combinations.

Abstract
Bortezomib, a proteasome inhibitor (PI), has shown efficacy in the treatment of newly diagnosed and relapsed light chain (AL) amyloidosis, and is often used in combination with cyclophosphamide and dexamethasone. Ixazomib is the first oral PI to be approved in routine practice but has not yet been evaluated in the upfront treatment setting. Newly diagnosed AL amyloidosis patients with measurable disease and adequate organ function were enrolled. The primary objective was to determine the hematologic response rate of ixazomib in combination with cyclophosphamide and dexamethasone. Treatment was given for 12 cycles, followed by ixazomib maintenance until progression. Thirty-five patients were included; their median age was 67 years, and 69% were male. Major organ involvement included heart (66%) and kidneys (54%). A median of 4 induction cycles (range, 1-12) were administered. The overall hematologic response to induction was 63% and included complete response in 11.4% and very good partial response in 37.1% of patients. One patient was upstaged to complete response during maintenance. The most common reason for going off study was the institution of alternate therapy (61%). With a median follow-up of 29.7 months for the living patients, the 2-year progression-free survival and overall survival were 74% and 78%, respectively. The median time to alternate therapy was 7.5 months. Grade ≥3 hematologic and nonhematologic adverse events occurred in 23% and 49% of patients. Given ixazomib’s favorable toxicity profile, which is an important advantage for the typically frail AL population, further evaluation of ixazomib in other combinations in the upfront setting is warranted. This trial was registered at www.clinicaltrials.gov as #NCT01864018.
Introduction
Light chain (AL) amyloidosis is a clonal plasma cell disorder characterized by secretion of light chains with amyloidogenic properties. These abnormal light chains misfold and deposit in the extracellular space as highly organized material termed amyloid.1 Amyloid is resistant to degradation by naturally occurring proteolysis mechanisms, and its gradual accumulation leads to organ dysfunction and death. In addition, precursor protein toxicity has been implicated as another mechanism for organ damage,2-6 which may explain the accelerated deterioration in organ function in AL amyloidosis compared with other forms of systemic amyloidosis.7 All therapies available for AL amyloidosis aim at the clonal plasma cell disorder, to reduce or eliminate the supply of the amyloidogenic light chains.8 Traditionally, these therapies have been adopted from the treatment landscape of multiple myeloma (MM), a more common plasma cell disorder, given the fundamental similarities between the 2 diseases. However, any treatment choice should balance benefit against toxicity. In AL amyloidosis, this is particularly important given the inherent organ dysfunction, leading to poor treatment tolerance, particularly in patients with advanced organ impairment.9
Bortezomib, the first-in-class proteasome inhibitor (PI) in use, has shown remarkable results in AL amyloidosis,10-13 likely due to the heightened sensitivity of AL cells to proteasome inhibition.5 Therefore, bortezomib is considered an integral part of first-line therapy in AL amyloidosis, with the most used regimen being cyclophosphamide, bortezomib, and dexamethasone (CyBorD).11,14 Most recently, CyBorD in combination with daratumumab has become the new standard of care for newly diagnosed AL amyloidosis.15 However, neuropathy related to bortezomib remains a challenge as peripheral and/or autonomic neuropathy occurs in approximately one-fifth of AL patients16 ; for these patients, bortezomib should be given with caution, at lower dose, or omitted altogether. Bortezomib can also increase cardiac toxicity in patients with advanced cardiac disease, and lower doses of bortezomib were suggested in this patient population.8,17,18 Ixazomib is the first oral PI introduced in the clinic and is currently approved in combination with lenalidomide and dexamethasone for the treatment of patients with MM who have received at least 1 prior therapy. Ixazomib was tested in relapsed refractory AL patients with promising results and a low toxicity profile.19,20 Herein, we present a phase 2 study assessing the safety and efficacy of ixazomib in combination with cyclophosphamide and dexamethasone in previously untreated AL amyloidosis.
Methods
Study design and objectives
This study is a single-arm, phase 2 study that was conducted in parallel with a separate cohort of patients with untreated MM, the results of which have been previously published.21 The primary objective of the study was to determine the hematologic response rate of ixazomib, used in combination with cyclophosphamide and dexamethasone, in patients with previously untreated AL. The secondary objectives were: (1) to determine the organ response rate; (2) to determine progression-free survival (PFS) and overall survival (OS); and (3) to determine the toxicities associated with ixazomib in combination with cyclophosphamide and dexamethasone. The study was performed in accordance with the provisions of the Declaration of Helsinki, the International Conference on Harmonisation, and the Guidelines for Good Clinical Practice, and with approval of the Mayo Clinic Institutional Review Board. The study was registered at www.clinicaltrials.gov as #NCT01864018.
Patients
Newly diagnosed patients, aged ≥18 years, with a biopsy-proven AL amyloidosis, with organ involvement requiring therapy, were enrolled. Patients had to have adequate hematologic function (absolute neutrophil count ≥1000/mm3, platelet count ≥75 000/mm3, and hemoglobin level ≥8.0 g/dL), adequate organ function (creatinine clearance ≥30 mL/min, total bilirubin level ≤1.5 × upper limit of normal, and alanine aminotransferase/aspartate aminotransferase levels ≤3 × upper limit of normal), and an Eastern Cooperative Oncology Group performance status score of 0 to 2. Patients were excluded if they had severe organ involvement, defined as alkaline phosphatase level >750 U/L or N-terminal pro–B-type natriuretic peptide levels ≥7500 ng/L. Patients had to have measurable disease, defined as difference between involved and uninvolved free light chain ≥5 mg/dL and abnormal serum immunoglobulin free light chain ratio. Also excluded were patients receiving systemic treatment with strong cytochrome P450 1A2 inhibitors or strong inhibitors/inducers of cytochrome P450 3A within 14 days for comorbidities or severe preexisting illness that, in the treating physician’s opinion, could interfere with oral absorption and/or tolerance of ixazomib.
Treatment and response assessment
Treatment consisted of ixazomib 4 mg days 1, 8, and 15; cyclophosphamide 500 mg by mouth weekly, and dexamethasone 40 mg weekly for 12 cycles (28-day cycle), followed by ixazomib maintenance at the last tolerated dose until progression. Ixazomib dose modifications for toxicity were made with successive reductions in its dose to 3 mg weekly, 2.3 mg weekly, and 2.3 mg every other week, followed by discontinuation if the lowest dose level was not tolerated. Cyclophosphamide dose modification included reduction to 400 mg and 200 mg before discontinuation. Dexamethasone dose modification included dose decrease to 20, 12, and 4 mg before discontinuation. Prophylactic antiemetic agents (prochlorperazine, ondansetron, and/or lorazepam) were recommended before each dose of ixazomib. Prophylactic antidiarrheal agents were not used; however, administration of antidiarrheal agents was allowed after infectious causes were excluded. Patients could choose to have hematopoietic stem cells collected for future use at any time after 3 cycles of initial therapy. Patients came off study if they experienced progressive disease, had unacceptable adverse events (AEs), refused to continue participation, or received a subsequent line of therapy. We used the consensus criteria for hematologic and cardiac response22 and the proposed revised renal response criteria23 for analysis. Responses were assessed every cycle.
Statistical analysis
The primary end point was the rate of hematologic response, where a success was defined as complete response (CR), very good partial response (VGPR), or partial response (PR) noted as the objective status on 2 consecutive evaluations during induction therapy. The one-stage binomial design required 33 evaluable patients to test the null hypothesis that the true hematologic response rate in this patient population is at most 30% vs the alternative hypothesis that it is at least 50%, with 85% power and 9% type I error. OS was defined as the time from study entry to death due to any cause. PFS was defined as the time from study entry to date of documentation of hematologic progression24 or death due to any cause. Time to alternative therapy was calculated from study entry until recipient of second-line therapy, regardless of the cause. Survival analysis was performed by using the Kaplan-Meier method. AEs were assessed using Common Terminology Criteria for Adverse Events version 4.0.
Results
Thirty-six patients were enrolled between May 2017 and May 2020. One patient was deemed ineligible and was removed from further analysis, and 35 patients were included in the analysis. The baseline characteristics of the study participants are listed in Table 1. The median age was 67, and 24 patients (69%) were male. Most patients had an Eastern Cooperative Oncology Group performance status score of 0 (46%) or 1 (49%). Heart involvement was the most involved organ (66%) followed by renal involvement (54%). The median difference between involved and uninvolved free light chain was 29 mg/dL. Mayo 2012 AL amyloidosis stage I-II and III-IV were assigned to 51% and 49% of patients, respectively. Data were frozen as of August 12, 2021. Across all study participants at data cutoff, 5 (14.3%) patients had progressed (2 hematologic progressions, 3 organ progressions) and 28 (80%) were alive, with a median follow-up of the living patients of 29.7 months (range, 1.6-47.9 months). Two patients (6.1%) remain on therapy; reasons for drug discontinuation were alternative treatment (n = 20 [61%]), AEs (n = 4 [12%]), disease progression while on treatment (n = 2 [6%]), withdrawal of patient consent (n = 2 [6%]), death on study (n = 1 [3%]), completion of therapy (n = 1 [3%]), and other (n = 3 [9%]).
Baseline characteristics of the entire cohort (N = 35)
| Characteristic | Value |
|---|---|
| Age, median (range), y | 67 (38-78) |
| Male | 24 (69%) |
| Race, white | 35 (100%) |
| ECOG performance status score | |
| 0 | 16 (46%) |
| 1 | 17 (49%) |
| 2 | 2 (6%) |
| Eligible for autologous stem cell transplant | 29 (85%) |
| Involved organs | |
| Cardiac | 23 (66%) |
| Renal | 19 (54%) |
| Nerve | 6 (17%) |
| Hepatic | 4 (11%) |
| >1 organ | 15 (43%) |
| Lambda restricted | 26 (74%) |
| BMPCs, median (range), % | 9 (<5%-30%) |
| dFLC, median (range), mg/dL | 29.0 (5.0-109) |
| Serum creatinine, median (range), mg/dL | 1.1 (0.6-1.9) |
| 2012 Mayo AL amyloidosis stage, I/II/III/IV, % | 20/31.4/22.9/25.7 |
| FISH abnormalities (n = 28)* | |
| t(11;14) | 50% |
| del(13q)/monosomy 13 | 43% |
| Trisomies | 32% |
| gain(1q) | 14% |
| del(17p)/monosomy 17 | 11% |
| t(4;14) | 4% |
| t(14;20) | 4% |
| >1 abnormality | 61% |
| Characteristic | Value |
|---|---|
| Age, median (range), y | 67 (38-78) |
| Male | 24 (69%) |
| Race, white | 35 (100%) |
| ECOG performance status score | |
| 0 | 16 (46%) |
| 1 | 17 (49%) |
| 2 | 2 (6%) |
| Eligible for autologous stem cell transplant | 29 (85%) |
| Involved organs | |
| Cardiac | 23 (66%) |
| Renal | 19 (54%) |
| Nerve | 6 (17%) |
| Hepatic | 4 (11%) |
| >1 organ | 15 (43%) |
| Lambda restricted | 26 (74%) |
| BMPCs, median (range), % | 9 (<5%-30%) |
| dFLC, median (range), mg/dL | 29.0 (5.0-109) |
| Serum creatinine, median (range), mg/dL | 1.1 (0.6-1.9) |
| 2012 Mayo AL amyloidosis stage, I/II/III/IV, % | 20/31.4/22.9/25.7 |
| FISH abnormalities (n = 28)* | |
| t(11;14) | 50% |
| del(13q)/monosomy 13 | 43% |
| Trisomies | 32% |
| gain(1q) | 14% |
| del(17p)/monosomy 17 | 11% |
| t(4;14) | 4% |
| t(14;20) | 4% |
| >1 abnormality | 61% |
BMPC, bone marrow plasma cells; dFLC, difference between involved to uninvolved light chains; ECOG, Eastern Cooperative Oncology Group.
Four patients had insufficient clonal plasma cells for testing; 3 patients did not have fluorescence in situ hybridization (FISH) testing performed.
Hematologic response, organ response, and survival
Hematologic response at 3, 6, and 12 months is depicted in Figure 1. The overall hematologic response at 3 and 6 months was 54.3% and 62.9%, with VGPR/CR rates at the 3 and 6 months’ time points of 22.9% and 45.8%, respectively. The overall response rate at 12 months (end of induction) was 62.9% (n = 22) with hematologic CR, VGPR, PR, and no response achieved in 11.4%, 37.1%, 14.3%, and 37.1% of the study population. The median time to hematologic response was 1 month, and the median time to best response was 2 months. The median time to VGPR/CR and to CR was 1.9 and 8.6 months. One patient who achieved VGPR during the initial first 12 months was upstaged to CR during maintenance. Organ responses were seen in a small proportion of patients. Cardiac response was attained in 13% of cardiac-evaluable patients (n = 23), renal response was achieved in 32% of renal-evaluable patients (n = 19), and 25% of hepatic-evaluable patients (n = 4) attained a response. Cardiac responses were seen in 2 patients achieving hematologic VGPR and 1 patient with hematologic CR. Renal responses were seen in 3 patients who achieved hematologic CR, 2 patients achieving hematologic VGPR, and 1 patient who attained hematologic PR. One liver response was seen in a patient achieving hematologic PR.
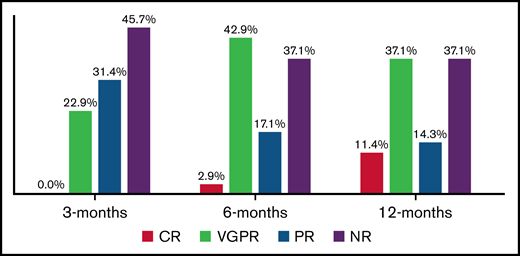
Hematological response rate at 3, 6, and 12 months time points. NR, no response.
Hematological response rate at 3, 6, and 12 months time points. NR, no response.
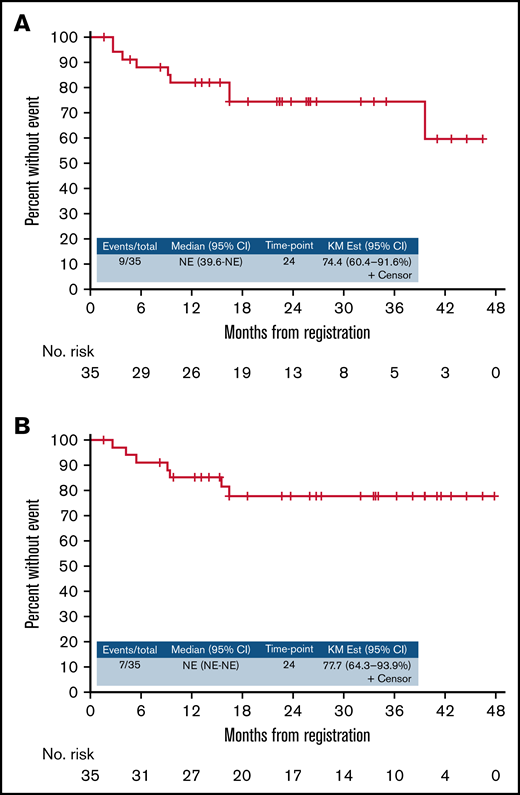
The median PFS was not reached (95% confidence interval, 39.6 months-not reached), with a 2-year PFS of 74.4% (Figure 2A). The median OS was not reached either, with a 2-year OS of 77.7% (Figure 2B). During follow-up, 7 patients died: 3 patients died due to disease progression, 2 died of disease progression at subsequent therapy, 1 died of hypoxemic respiratory failure after autologous stem cell transplantation, and 1 died of unknown cause.
Response by fluorescence in situ hybridization genetics
There was no difference in response to ixazomib in combination with cyclophosphamide and dexamethasone in relation to t(11;14) status. Patients with t(11;4) had similar response rates as non–t(11;14) patients (64.3% vs 57.1%; P = .69). In addition, depth of response was also similar between groups (VGPR or better, 35.7% vs 50%; P = .44). There was no difference in response rate according to chromosome 13 abnormalities or presence of trisomies. Of the 4 patients with high-risk abnormalities determined via fluorescence in situ hybridization [del 17p, t(4:14), or t(14;20)], 2 patients achieved hematologic response (CR and VGPR each).
Dose intensity and AEs
The median number of induction cycles was 4 (range, 1-12). Five patients completed 12 induction cycles and proceeded to ixazomib maintenance, with maintenance ranging from 1 to 17 cycles. Table 2 lists the total number of cycles administered and the number of patients requiring dose reductions. Treatment delays occurred 7 times among 6 patients. Treatment delay was per protocol in 3 patients and for other reasons in 4 patients. Any AE of any relation to study intervention was reported in 97% of patients. Table 3 lists the percentage of AEs by severity and relation to study drugs, and separated into hematologic and nonhematologic AEs. Any AE grade ≥3 regardless of attribution occurred in 57% of patients (46% for AEs that were at least possibly related to study drugs). Grade ≥3 nonhematologic AEs regardless of attribution occurred in 49% of patients, and grade ≥3 hematologic AEs occurred in 23% of patients. AEs that were at least possibly attributed to the study drugs are presented according to system and grade in supplemental Table 1.
Treatment administration
| Variable | Ixazomib | Cyclophosphamide | Dexamethasone |
|---|---|---|---|
| No. of cycles administered | 255 | 219 | 219 |
| Median dose per cycle | 12 | 2000 | 160 |
| Range | 0-12 | 0-2000 | 0-160 |
| No. of patients with adjustments | 5 | 3 | 10 |
| Total reductions | 6 | 4 | 12 |
| Reasons for adjustments | |||
| Investigations | 1 | 0 | 0 |
| Gastrointestinal disorders | 0 | 0 | 3 |
| General disorders and administration site conditions | 0 | 0 | 4 |
| Metabolism/nutrition disorders | 0 | 0 | 1 |
| Musculoskeletal-connective tissue disorders | 0 | 0 | 1 |
| Nervous system disorders | 3 | 0 | 0 |
| Per protocol | 1 | 1 | 0 |
| Other | 1 | 3 | 3 |
| Variable | Ixazomib | Cyclophosphamide | Dexamethasone |
|---|---|---|---|
| No. of cycles administered | 255 | 219 | 219 |
| Median dose per cycle | 12 | 2000 | 160 |
| Range | 0-12 | 0-2000 | 0-160 |
| No. of patients with adjustments | 5 | 3 | 10 |
| Total reductions | 6 | 4 | 12 |
| Reasons for adjustments | |||
| Investigations | 1 | 0 | 0 |
| Gastrointestinal disorders | 0 | 0 | 3 |
| General disorders and administration site conditions | 0 | 0 | 4 |
| Metabolism/nutrition disorders | 0 | 0 | 1 |
| Musculoskeletal-connective tissue disorders | 0 | 0 | 1 |
| Nervous system disorders | 3 | 0 | 0 |
| Per protocol | 1 | 1 | 0 |
| Other | 1 | 3 | 3 |
Frequency of AEs (N = 35)
| Grouping | Regardless of attribution | At least possibly related |
|---|---|---|
| AEs grade ≥1 | 34 (97%) | 33 (94%) |
| AEs grade ≥3 | 20 (57%) | 16 (46%) |
| AEs grade ≥3 hematologic | 8 (23%) | 6 (17%) |
| AEs grade ≥3 nonhematologic | 17 (49%) | 13 (37%) |
| AEs grade ≥4 | 8 (23%) | 4 (11%) |
| AEs grade ≥4 hematologic | 3 (9%) | 2 (6%) |
| AEs grade ≥4 nonhematologic | 6 (17%) | 3 (9%) |
| AEs grade 5 | 1 (3%) | 0 (0%) |
| AEs grade 5 non-hematologic | 1 (3%) | 0 (0%) |
| Grouping | Regardless of attribution | At least possibly related |
|---|---|---|
| AEs grade ≥1 | 34 (97%) | 33 (94%) |
| AEs grade ≥3 | 20 (57%) | 16 (46%) |
| AEs grade ≥3 hematologic | 8 (23%) | 6 (17%) |
| AEs grade ≥3 nonhematologic | 17 (49%) | 13 (37%) |
| AEs grade ≥4 | 8 (23%) | 4 (11%) |
| AEs grade ≥4 hematologic | 3 (9%) | 2 (6%) |
| AEs grade ≥4 nonhematologic | 6 (17%) | 3 (9%) |
| AEs grade 5 | 1 (3%) | 0 (0%) |
| AEs grade 5 non-hematologic | 1 (3%) | 0 (0%) |
Subsequent therapy
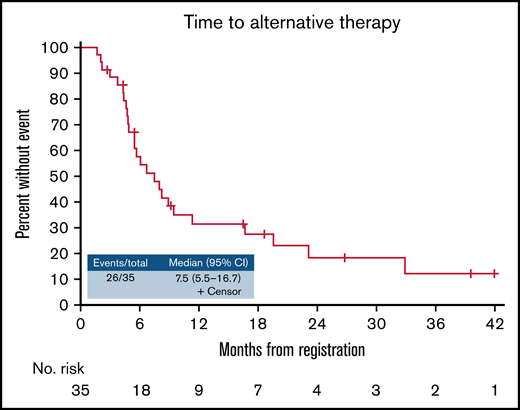
Twenty-six patients (74.3%) proceeded to a second-line therapy. Of these, 20 patients proceeded to second-line therapy to deepen their response (no response, n = 9; PR, n = 3; VGPR, n = 8), 2 patients proceeded to second-line therapy due to AE, one patient proceeded to second-line therapy due to disease progression, and 3 patients for other causes. Of the second-line therapies, 8 patients received autologous stem cell transplantation (1 patient following daratumumab induction), 6 patients proceeded to daratumumab and dexamethasone combination, 6 patients to daratumumab in combination with bortezomib and dexamethasone, 4 patients to bortezomib-based therapy, and 3 patients proceeded with other forms of therapy. The median time from initiation of study treatment to initiation of second-line therapy among these 26 patients was 7.5 months (95% confidence interval, 5.5-16.7) (Figure 3). The hematologic response to study treatment was CR in 2 (4%) patients, VGPR in 9 (35%) patients, PR in 4 (15%) patients, and no response in 11 (42%) patients. Response to second-line therapy was available for 25 of 26 patients. The overall hematologic response to second-line therapy was 88% and included CR in 32% of patients, VGPR in 52% of patients, and PR in 4% of the patients. Three patients did not achieve a response to second-line therapy. Of these 25 response-evaluable patients, 17 (68%) had response improvement compared with the study treatment, 7 (28%) had same response level as with the study treatment combination, and 1 patient (4%) lost depth of response (CR to VGPR). Of the 4 patients who received bortezomib-based therapy as a second-line therapy, 2 patients received >4 cycles on the study protocol (and thus could be assessed for depth of response). These 2 patients had response improvement with CyBorD (PR to VGPR and VGPR to CR).
Discussion
In this phase 2 study, we have shown that the combination of ixazomib, cyclophosphamide, and dexamethasone is active in newly diagnosed AL amyloidosis, with hematologic response seen in 63% of patients. However, the hematologic CR rate was low (11.4%), and many patients proceeded with alternate therapy to seek deeper hematologic response. Importantly, therapy was well tolerated in the overall frail AL population, with dose modifications and therapy discontinuation seen only in a minority of patients. The toxicity profile in this study is similar to what has been reported in prior studies with ixazomib in AL amyloidosis,19,20 although the low number of patients in the current and prior studies and fundamental differences between these studies may explain the variability in frequency of reported side effects. This study also had a maintenance arm with single-agent ixazomib; 5 patients were treated through this treatment phase. This is a novel approach in amyloidosis, being tested as well in the ANDROMEDA (A Randomized Phase 3 Study to Evaluate the Efficacy and Safety of Daratumumab in Combination With Cyclophosphamide, Bortezomib and Dexamethasone [CyBorD] Compared to CyBorD Alone in Newly Diagnosed Systemic AL Amyloidosis) study15 and follows a common practice in MM. However, the potential benefits of maintenance in AL amyloidosis should be preferably explored in a randomized fashion. This study supports further evaluation of the role of ixazomib in the management of AL amyloidosis, including in the upfront setting.
Bortezomib has been the backbone of the initial therapy for AL amyloidosis for approximately a decade.11,14,25 Data on the efficacy and safety of bortezomib in the upfront setting are available mostly from retrospective studies,11,13,26,27 as well as from one small phase 3 study in which bortezomib combined with melphalan and dexamethasone (BMDex, n = 53) was compared in a randomized manner vs melphalan and dexamethasone (MDex, n = 56).10 In that study, the overall hematologic response rate of BMDex was 79%, with VGPR or better reported in 55% of patients. In the 2 largest retrospective studies of unselected patient populations, the overall hematologic response rate to CyBorD was 60% to 65%, with VGPR or better reported in 43% to 45% of patients.11,13 A head-to-head comparison between the aforementioned studies and the current one is problematic given the differences between studies in design, baseline participants’ characteristics, treatment components, and treatment schedule. The ixazomib-based regimen is distinguished by an all-oral, well-tolerated regimen and should be specifically preferred in instances in which bortezomib is unsafe for use such as in the presence of preexisting neuropathy.
Sensory neuropathy at least possibly related to study drugs was seen in 34.3% of patients (12 of 35 patients) (supplemental Table 1), the vast majority being grade 1 (8 of 35 [22.9%]); grade 3 sensory neuropathy was seen in 1 patient only. These rates were comparable to our experience with this regimen in patients newly diagnosed with MM.21 In comparison, a BMDex regimen in AL amyloidosis resulted in sensory neuropathy of any grade in almost all patients (98%), with grade 3/4 sensory neuropathy in 13.2% of patients. This indicates that ixazomib-based therapy is characterized by lower neurotoxicity than bortezomib, which is particularly important in AL amyloidosis, where nerve involvement is seen in approximately one-quarter of patients.16 The most common side effects of ixazomib, cyclophosphamide, and dexamethasone were gastrointestinal, particularly nausea and constipation, which were noted in large portion of patients (40% both) but were typically limited to grade 1/2. Diarrhea was seen in 28.6% of patients, typically as grade 1 and 2. The use of prophylactic antiemetic agents in this study may have resulted in a better gastrointestinal side effect profile. The study regimen is also characterized by low cardiac toxicity, with very few patients experiencing cardiovascular toxicity (including heart failure and arrhythmias), and because the heart is the most involved organ in AL amyloidosis, this is an important advantage. Cardiac toxicity has been reported in a higher proportion for other PIs, bortezomib28 and particularly carfilzomib.29
This study was conducted in era of major changes in care for AL patients. First, given the importance of achieving deep and rapid hematologic response,22 our practice is to change therapy within several months if VGPR is not reached.8 In addition, during trial enrollment, daratumumab was increasingly used as salvage therapy given its low toxicity and promising results in the relapsed refractory setting.30 These factors were major determinants for the high proportion of patients coming off study for alternate therapy within a median of nearly 6 months from study entry. Another major practice change that affects the study results’ interpretation is the adoption of daratumumab in combination with CyBorD as the new standard of care for newly diagnosed AL patients given its superior response rate (particularly complete response rate) compared with CyBorD.15 One of the considerations that can be drawn from this study is the replacement of bortezomib with ixazomib when combined with daratumumab in the upfront setting. Such a change possibly will not significantly affect response rate but can increase treatment tolerability, especially among those patients who are expected to have poor treatment tolerance such as those with advanced cardiac stage or neuropathy.25,28,31,32 These patient populations are extremely vulnerable to treatment toxicity, leading to therapy interruption and/or discontinuation.
The major limitations of this study are the small number of patients, which is typical for rare disease, such as AL amyloidosis, and the change in practice in recent years, which requires re-framing of the study results to the current treatment landscape.
In conclusion, the combination of ixazomib, cyclophosphamide, and dexamethasone is active in newly diagnosed AL amyloidosis. It provides an effective regimen while minimizing side effects, an important advantage in AL amyloidosis given poorer treatment tolerance with advanced organ dysfunction. In the era of upfront use of daratumumab, the combination of ixazomib and daratumumab may offer a more tolerable regimen with a safer toxicity profile and should be explored in future studies.
Authorship
Contribution: E.M. was responsible for patient recruitment and management, acquisition, analysis and data interpretation, and drafting the manuscript; M.A.G., F.K.B., N.L., P.L.B., A.F., Y.L.H., M.H., W.G., M.Q.L., P.K., M.S., J.T.L., R.W., S.R.H., R.S.G., D.D., T.V.K., A.D., and S.V.R. were responsible for patient recruitment and management; B.R.L. and P.O. were responsible for acquisition, analysis and data interpretation, and drafting the manuscript; D.K.H. and E.E.B. were responsible for patient management; S.K.K. was responsible for concept and study design, patient recruitment and management, acquisition, analysis and data interpretation, and drafting the manuscript; and all authors approved the final version of the manuscript.
Conflict-of-interest disclosure: E.M. reports honorarium from Janssen and consultation fee from Protego (fee paid to institution). M.A.G. served as a consultant for Millennium Pharmaceuticals; and received honoraria from Celgene, Millennium Pharmaceuticals, Onyx Pharmaceuticals, Novartis, GlaxoSmithKline, Prothena, Ionis Pharmaceuticals, and Amgen. P.L.B. received honoraria from Janssen, Novartis, GSK, Oncopeptides, and Amgen. N.L. served on the advisory board for Takeda Pharmaceuticals. A.D. reports research funding from Celgene, Millennium Pharmaceuticals, Pfizer, and Janssen; and has received a travel grant from Pfizer. M.Q.L. reports research funding from Celgene. P.K. is a principal investigator of research studies for which Mayo Clinic has received funding from AbbVie, Takeda, Sanofi, Janssen, Karyopharm, GlaxoSmithKline, Regeneron Pharmaceuticals, Ichnos Sciences, and Amgen; and has served on the medical advisory board meetings of Sanofi, Pharmacyclics, BeiGene, Cellectar, GSK, X4, and Karyopharm. S.K.K. received research funding for clinical trials to the institution from AbbVie, Amgen, BMS, CARsgen, Janssen, AstraZeneca, Novartis, Roche-Genentech, Takeda, TeneoBio, and Molecular Templates; and received consulting/advisory board participation (with no personal payments) from AbbVie, Amgen, BMS, Janssen, Roche-Genentech, Takeda, AstraZeneca, Bluebird Bio, Epizyme, Secure Biotherapeutics and (with personal payment) Oncopeptides, BeiGene, and Antengene. The remaining authors declare no competing financial interests.
Correspondence: Shaji K. Kumar, Division of Hematology, Mayo Clinic, 200 First St, SW, Rochester, MN 55905; e-mail: kumar.shaji@mayo.edu.

