

TO THE EDITOR:
The definition of surrogacy for a clinical end point has been precisely delineated, by the National Cancer Institute Dictionary of Cancer Terms, for example. It is an indicator used in place of another to tell whether a treatment works and may be used instead of stronger indicators, such as longer overall survival (OS) in cancer research. Any conclusion about whether an end point is a valid surrogate usually depends on the type of cancer, line of therapy, and type or class of drug. Overall, surrogacy validation commonly requires extensive patient data to be collected, both at the individual and trial levels, and requires formal statistical demonstration.
Given its indolent course and treatment improvement over recent years, it has become more and more challenging, if not unachievable, to demonstrate OS prolongation after first-line therapy in follicular lymphoma (FL). Additional end points that could serve as surrogates for OS and could provide earlier access to newer therapies in the disease or could expedite clinical trials are eagerly awaited. Recently published data have demonstrated how early progression of disease after first-line immunochemotherapy in patients with FL is associated with significantly shorter subsequent OS.1-3 Although no formal demonstration that progression of disease (POD) occurring 12, 18, or 24 months (ie, POD12, POD18, or POD24) after initiation of the induction regimen in FL can be considered to be surrogates for OS, there is a common drift in the belief of physicians that an experimental treatment decreasing the rate of early events would indicate a prolonged long-term OS benefit with longer follow-up.3,4
From a proper statistical definition, as originally defined by Prentice,5 surrogate end points must fulfill 2 main criteria. First, there must be a strong association between the surrogate (eg, early progression) and the true end point (eg, OS; the individual-level surrogacy). Second, there must be a strong association between the effect of a given treatment on the surrogate (eg, effect of a treatment X on POD24) and the true end point (eg, effect of treatment X on OS; the trial-level surrogacy). The first criterion is usually easily fulfilled by most end points considered to be potential surrogates for survival, but the second criterion for the true end point may be far from fulfilled.
We recently confirmed with a long-term follow-up that progression-free survival (PFS) was still significantly prolonged when using rituximab maintenance, and we also reproduced the strong correlation between POD24 and OS in the PRIMA study.6 However, PFS prolongation has not translated into a longer OS in the maintenance arm after 9 years of follow-up.7 Based on these findings, we tried to gain a better insight into the singular relationship between an early event or progression and subsequent survival in patients with FL treated by upfront immunochemotherapy.
PRIMA was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. The study protocol and amendments were approved by local and national ethics committees, according to the laws of each country. Patients provided written informed consent. Among the 1193 patients in the induction analysis population of the PRIMA study, 22 died within the first 2 years without documented lymphoma progression, and 33 were lost to follow-up and were subsequently removed from the analysis set to allow for POD24 assessment. Of the 1138 remaining patients, 998 in partial or complete response after induction were randomized between rituximab maintenance (n = 495) or observation (n = 503). The patients who were not randomized (n = 140) were removed from subsequent analyses because the purpose of the study was to evaluate the effect of maintenance or observation on different clinical end points (see patient flow in Figure 1). POD24 was defined as progression within the 24 months after registration in the PRIMA study. OS after the risk-defining event was defined as OS since the early progression date for patients experiencing POD24 or 24 months after registration for the others.
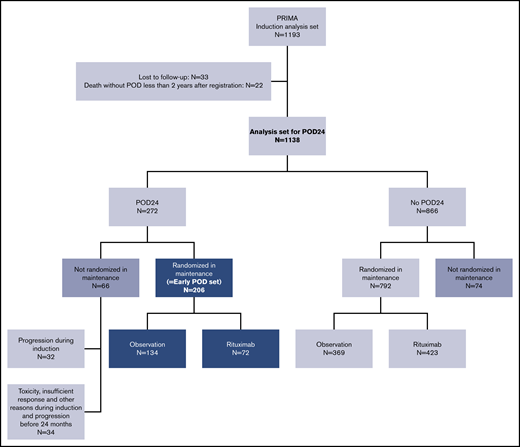
Patient flow. The early POD set encompassing the patients who progressed during the first 24 months and were randomized in the PRIMA study is enclosed in dark blue boxes. The set of patients added in the sensitivity analysis, with randomization in a pseudo-arm at registration, is enclosed in dark gray boxes.
Patient flow. The early POD set encompassing the patients who progressed during the first 24 months and were randomized in the PRIMA study is enclosed in dark blue boxes. The set of patients added in the sensitivity analysis, with randomization in a pseudo-arm at registration, is enclosed in dark gray boxes.
Rituximab maintenance translated into a significantly lower number (n = 72) of patients experiencing POD24 compared with patients (n = 134) in the observation arm (14.5% vs 26.6%, P < .001; χ2 test; Figure 2A). However, long-term follow-up for the 998 randomized patients in the analysis set revealed no OS prolongation in patients treated with rituximab maintenance compared with controls with no maintenance (8-year survival 85.4% vs 84.7%, P = .84; Figure 2B).7

POD24, OS, and survival after progression according to treatment arm. (A) POD24 by treatment arm. (B) OS by treatment arm, measured from registration. (C) OS according to POD24 status for the whole cohort. (D) OS according to POD24 status by treatment arm.
POD24, OS, and survival after progression according to treatment arm. (A) POD24 by treatment arm. (B) OS by treatment arm, measured from registration. (C) OS according to POD24 status for the whole cohort. (D) OS according to POD24 status by treatment arm.
To understand why POD24 improvement did not translate into prolonged OS in the PRIMA study, we compared OS from registration for those patients experiencing POD24 with those without POD24 for the whole cohort (Figure 2C) and by randomization arm (Figure 2D). Updated follow-up of the study confirmed the strong correlation between POD24 and subsequent OS: 5-year OS was 76.2% (95% CI, 69.6-81.5) for patients with early progression compared with 97.2% (95% CI, 95.8-98.1) for the others (Figure 2C). The lack of OS difference with long-term follow-up between the 2 arms of treatment, despite the lower rate of POD24 with maintenance rituximab, suggests that OS is shorter after early progression in the maintenance arm than in the observation arm, which was confirmed to have 5-year OS of 69.5% (95% CI, 57.1-78.9) compared with 79.7% (71.8-85.6), respectively (Figure 2D). Similar results were observed when OS after the risk-defining event rather than from registration was considered (supplemental Figure 1). This finding should be interpreted with caution, because it does not mean that maintenance conveys an adverse outcome in cases of early progression. It probably only reflects that this smaller group of patients who progressed during maintenance are those with the most aggressive disease for whom the ultimate adverse outcome is unlikely to be affected by currently available therapeutic interventions. Indeed, and as previously reported in the long-term follow-up of the PRIMA study,7 complete and noncomplete response rates after second-line treatment were lower for early progressors in the rituximab maintenance arm than in the observation arm (39% v 56%; P = .029; supplemental Table 1). We also found that early progressors during maintenance exhibited a high FL International Prognostic Index score of 3 to 5 at diagnosis more frequently than early progressors in the observation arm, even though the difference did not reach statistical significance (61% vs 48%, respectively; P = .067; supplemental Table 2). We previously reported that the second line rituximab-based regimen was only slightly less frequently used in the maintenance arm than in the observation arm (73% vs 81%) and with no difference from other treatments such as stem cell consolidation.7 It is therefore unlikely that the difference in OS after relapse in early progressors according to treatment arm is attributable to the use of a less potent regimen for second-line therapy after early progression in the maintenance arm. Furthermore, no significant difference in histological transformation to high-grade lymphoma has been observed (supplemental Figure 2). Altogether, the shorter survival for POD24 patients in the immunotherapy maintenance arm is indeed related to a core subset of patients with poor disease characteristics, whatever the first-line therapy, not an effect of maintenance by itself. The worse prognosis of this patient subset is statistically diluted in the observation arm (where POD24 patients with better prognoses are admixed), explaining the overall more favorable outcome in this treatment arm.
Our study has one main limitation. Because patients were randomized to rituximab maintenance or observation 6 months after registration at the end of induction in the PRIMA study, analyses to study the effect of treatment on outcome after early progression could not take into account very early progressors during induction (n = 32) and patients who were not randomized because they had stable disease, treatment toxicity, or for other reasons, but progressed later on, before 24 months (n = 34; Figure 1). A strict definition of POD24 was therefore not applied for the purpose of evaluating treatment effect on surrogacy between POD24 and OS. It could explain why OS after early progression was not significantly different in the recently published work by Seymour and colleagues7 between the 2 treatment arms of the GALLIUM study compared with the present study. However, in a sensitivity analysis where the 140 patients who did not undergo randomization in the PRIMA study (Figure 1) were randomly assigned to a pseudoarm at inclusion (70 in the maintenance arm and 70 in the observation arm), the difference was still statistically significant (supplemental Figure 3). Another likely explanation is that follow-up in PRIMA is far longer than in GALLIUM and that OS curves separation may ultimately occur in GALLIUM with a poorer late outcome for early progressors after obinutuzumab-based immunotherapy. To test this hypothesis, we compared OS in POD24 patients according to treatment arm based on an earlier simulated study cutoff allowing for a 48-month median patient follow-up (compared with the 41-month median follow-up in GALLIUM). A significant OS difference was not observed anymore with this shorter follow-up in PRIMA (supplemental Figure 4) like what was observed in GALLIUM. Therefore, long-term follow-up of the GALLIUM study will be of utmost interest to assess late survival of early progressors.
So far, only a few studies have convincingly demonstrated surrogacy in indolent lymphoma. A 30-month complete response rate was shown to serve as a potential reliable surrogate for PFS in FL, but remains to be fully validated in recent trials and has not been evaluated as a surrogate for OS.8 In aggressive lymphomas where the course of disease is radically different from FL, surrogacy for OS has been much easier to assess and has been convincingly demonstrated for PFS in general and progression within 24 months after induction in particular.9
To summarize, extreme caution should be used when considering an early event as a marker for subsequent survival in indolent lymphoma. Indeed, if POD24 was a real and consistent surrogate end point for OS, the significant benefit of maintenance rituximab on POD24 for high-tumor-burden FL would have been expected to translate into significantly prolonged OS after 9 years of follow-up in the PRIMA cohort. Further studies based on long-term follow-up of randomized trials are needed to precisely understand relationships between treatment efficacy, early progression, and OS alteration. Early progression after immunochemotherapy, such as POD24, is therefore an excellent posttreatment prognostic indicator, but it does not meet requirements to be a surrogate end point to compare the efficacy of different treatments for hypothetical OS prolongation.
Original data are available by e-mail request to the corresponding author (emmanuel.bachy@chu-lyon.fr).
Acknowledgments:
PRIMA was sponsored by the Lymphoma Study Association (LYSA) and supported by F. Hoffmann-La Roche Ltd and Biogen Idec Ltd.
Contribution: E.B. and G.S. conceived of the study, performed the data analysis, and wrote the manuscript; and J.R.C. performed the data analysis and wrote the manuscript.
Conflict-of-interest disclosure: G.S. has received financial compensation for advisory board or consulting roles from Abbvie, Autolus, Celgene, Genmab, Gilead, Epizyme, Janssen, Karyopharm, Kite, Merck, Morphosys, Novartis, Roche, Servier, and Takeda, and for participation in educational events by Abbvie, Amgen, Celgene, Gilead, Janssen, Kite, Morphosys, Novartis, Roche, Servier, and Takeda. J.R.C. has received research grants from BMS, Nanostring, and Genentech, and financial compensation for serving on the advisory board of Janssen. E.B. has received research funding from Amgen and financial compensation for advisory board or consulting roles from Sanofi, Novartis, Amgen, Kite/Gilead, Roche, Beigene, and Celgene.
The current affiliation for G.S. is Memorial Sloan Kettering Cancer Center, New York, NY.
Correspondence: Emmanuel Bachy, Hematology Department, Lyon Sud Hospital, Pierre Bénite, France; e-mail: emmanuel.bachy@chu-lyon.fr.

