

Key Points
The risk of pregnancy in women with in situ vena cava filter is unknown and was evaluated in a cohort study and literature.
Only 20 pregnancies were identified; 1 published case with pre-existent filter perforation had uterine trauma and fetal loss.

Abstract
Patients with an inferior vena cava (IVC) filter that remains in situ encounter a lifelong increased risk of deep vein thrombosis and IVC filter complications including fracture, perforation, and IVC filter thrombotic occlusion. Data on the safety of becoming pregnant with an in situ IVC filter are scarce. The objective was to evaluate the risk of complications of in situ IVC filters during pregnancy. We performed a retrospective cohort study of pregnant patients with an in situ IVC filter from a tertiary center between 2000 and 2020. We collected data on complications of IVC filters and pregnancy outcomes. Additionally, we performed a systematic literature search in MEDLINE, Embase, and gray literature. We identified 7 pregnancies in 4 patients with in situ IVC filters with a mean time since IVC filter insertion of 3 years (range, 1-8). No complications of IVC filter occurred during pregnancy. Review of literature yielded five studies including 13 pregnancies in 9 patients. In 1 pregnancy a pre-existent, until then asymptomatic, chronic perforation of the vena cava wall by the IVC filter caused major bleeding and uterine trauma with fetal loss. Overall, the complication rate was 5%. It seems safe to become pregnant with an indwelling IVC filter that is intact and does not show signs of perforation, but because of the low number of cases, no firm conclusions about safety of in situ IVC filters during pregnancy can be drawn. We suggest imaging before pregnancy to reveal asymptomatic IVC filter complications.
Introduction
Inferior vena cava (IVC) filters were introduced in the 1970s to prevent thrombus migration from veins in the lower extremities to the pulmonary arteries causing potentially life-threatening pulmonary embolism (PE). Classic indications for IVC filter include acute venous thromboembolism (VTE, comprising deep vein thrombosis [DVT] and PE) when anticoagulant treatment is absolutely contraindicated, and recurrent VTE despite adequate anticoagulant therapy.1‐5 IVC filters are also reported to be used for so-called extended or relative indications including the prevention of recurrent PE in chronic thromboembolic pulmonary hypertension patients undergoing pulmonary endarterectomy.1‐3,5 If indicated, guidelines recommend the use of temporary retrievable IVC filters that are designed and intended to be removed after a short period, over the use of permanent nonretrievable filters.4
Complications of IVC filters have been reported in 7% to 22% of the nonpregnant population6,7 and in 9% to 42% of patients who had an IVC filter inserted during pregnancy.7‐9 Acute complications after IVC filter insertion include access site thrombosis (ie, iliac vein thrombosis), infection, bleeding, and perforation.2,10 Perforation of the vena cava wall by the IVC filter could be asymptomatic or require intervention when surrounding organs are involved. In the absence of anticoagulant therapy, IVC filters pose the risk of iatrogenic lower limb DVT and IVC filter thrombotic occlusion leading to IVC syndrome.2,10 Filter tilt of more than 15° after insertion is associated with higher PE rates and higher retrieval failure rates, especially when certain types of filters are used.11 Other IVC filter-related complications consist of filter migration of more than 2 cm and fracture and embolization of struts.2,11 These complications are mostly associated with longer indwelling times and often remain asymptomatic but contribute to decreased efficacy of the IVC filter and failure of retrieval with temporary filters.2,10 Retrieval failure was reported in 11% to 12% of nonpregnant7,12 and in 8% to 26% of pregnant patients,7‐9 with higher failure rates for prolonged time to first removal attempt. Because of the risk of these adverse events, insertion of an IVC filter should be considered with prudence and temporary IVC filters should be retrieved as soon as possible.5,13
Patients with an IVC filter that remains in situ encounter lifelong risks. This has significant implications for young women in particular. Studies evaluating long-term outcomes focus on postthrombotic syndrome, VTE recurrence, and mortality,14,15 and have shown an increased risk of DVT for patients with in situ IVC filter.14 There are very few data on the safety of becoming pregnant with an in situ IVC filter. A systematic review by Harris et al reported complications of IVC filter in 124 women who had an IVC filter inserted during pregnancy, but those who had an IVC filter before conception were excluded from the review.8 It is unclear whether pregnancy and labor could affect the anatomic configuration of the in situ IVC filter and cause complications. In this study, we aim to evaluate the safety of pregnancy in women with an in situ IVC filter.
Methods
Data collection
Retrospective cohort study by chart review.
We identified all women who became pregnant with an in situ IVC filter between 1 January 2000 and 1 January 2020 at 1 of the 2 locations of Amsterdam University Medical Centers (Academic Medical Center and Vrije Universiteit Medical Center). A search engine designed to search unstructured data (CTCue) was used. We searched for “vena cava filter,” “VCF,” or synonyms in electronic medical charts of female patients aged 18 to 45 years during the defined period. Anonymized sections of patients’ charts were screened for relevance. All investigators obtained full access to the medical charts after confirming (possible) eligibility. When a patient had an in situ IVC filter, patient’s chart was searched for notes on pregnancy until the end of the study period or until the patient had turned 45, underwent hysterectomy, or had died. Pregnant patients with an in situ IVC filter before conception were included. The following data were extracted from chart notes: age at insertion, date of insertion, indication, location, type, complications of IVC filter during pregnancy, performed imaging of IVC filter before and after pregnancy, thrombotic history, obstetric history, pregnancy outcome (duration, mode of delivery, condition, and birth weight of neonate), concomitant anticoagulation during pregnancy, and pregnancy-related VTE.
Literature search.
In addition, a comprehensive search of English language literature was performed in MEDLINE and Embase to identify studies that evaluated the safety of in situ IVC filters during pregnancy. The search was based on both Medical Subject Headings terms and alternative general key words “pregnancy” and “vena cava filter.” The search strategy can be found in supplemental Table 1. We also manually searched for studies presented as abstracts at conferences of the American Society of Hematology, International Society on Thrombosis and Haemostasis, European Congress on Thrombosis and Haemostasis, Society of Maternal Fetal Medicine, Society of Reproductive Investigation, American Thoracic Society, European Respiratory Society, European Society of Cardiology, Society of Interventional Radiology, and Cardiovascular and Interventional Radiological Society of Europe. No restrictions with regard to publication date were applied; the search was performed on 7 August 2020. Two reviewers (I.B. and A.G.) independently screened titles and abstracts of all studies. Full-text articles of potentially relevant studies were examined for eligibility. Studies presenting original data were included if (1) the study population included at least 1 patient who had a pregnancy with in situ IVC filter and (2) the following outcomes were reported: IVC filter complications during pregnancy, obstetric outcomes, or recurrent VTE. All references of included studies were manually searched to identify articles that had not been identified. Quality of included studies was critically appraised for by I.B. and A.G. using the Joanna Briggs Institute tool for case series and case reports. Risk of bias assessment was not conducted because case series and case reports are by nature prone to bias. Moreover, risk of bias assessment was considered not of value for cohort studies when data of only a single patient was extracted. The following data were extracted from included studies: age at insertion, date of insertion, indication, location, type, complications of IVC filter during pregnancy, thrombotic history, obstetric history, pregnancy outcome (duration, mode of delivery, condition and birth weight of neonate), concomitant anticoagulation during pregnancy, and pregnancy-related VTE.
Study outcomes
The primary outcome of this study consisted of complications of IVC filter during pregnancy or diagnosed up to 6 weeks postpartum and included migration (>2 cm), tilt (>15°), or fracture of the IVC filter, penetration (>3 mm) of the vena cava wall, or IVC filter thrombosis or bleeding caused by IVC filter complications. Secondary outcomes were mode of delivery and pregnancy-related (during pregnancy or up to 6 weeks postpartum) recurrent VTE.
Statistical analysis
The primary and secondary outcomes were reported for the cohort and for the literature review separately. Descriptive analysis was performed using SPSS BMI version 26. Categorical data were presented as percentages and continuous variables as means with range.
Ethics
The study protocol was approved by the institutional review board of Amsterdam UMC, University of Amsterdam. The study re-used clinical data for research purposes, therefore need for written informed consent from patients was waived by the institutional review board under contemporary regulations.
Results
Identification cohort
The CTCue search in the medical charts between 1 January 2000 and 1 January 2020 yielded 487 records, of which 115 were female patients aged 18 to 45 years (Figure 1). Of these patients, 57 had an IVC filter inserted. The IVC filter was retrieved in 25 patients; 32 patients had an IVC filter that had remained in situ. Among the latter, 4 patients had become pregnant after IVC filter insertion, for a total of 7 pregnancies. Five patients with an in situ IVC filter were no longer under the care of our hospital 5 to 10 years ago, but might, based on age, have become pregnant and were considered lost to follow-up.
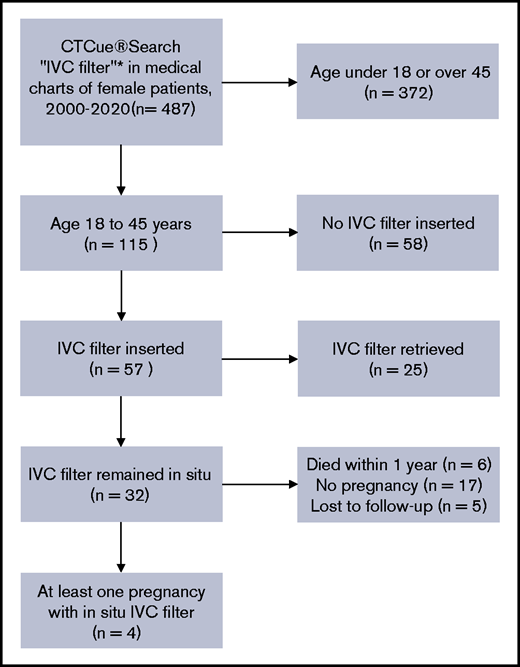
Flowchart selection of cohort. *Key words search: “vena cava filter,” “VCF,” and Dutch synonyms.
Flowchart selection of cohort. *Key words search: “vena cava filter,” “VCF,” and Dutch synonyms.
Cohort findings
Characteristics and outcomes of patients who became pregnant with an in situ IVC filter are summarized in Table 1. Mean age at IVC filter insertion was 27 years (range, 21-31). One patient had a retrievable (OptEase) IVC filter inserted because surgery for intra-abdominal bleeding was indicated 1 week after acute PE. Retrieval of the IVC filter was attempted 4 weeks later, but failed as the tip of the IVC filter was embedded into the IVC wall. During this procedure, the IVC filter was slightly twisted. In this patient, the presence of an in situ IVC filter was the major indication for therapeutic dose anticoagulants, which was continued during her subsequent pregnancy. Two patients had IVC filters inserted before pulmonary endarterectomy because of chronic thromboembolic pulmonary hypertension. One of these patients had a permanent TrapEase filter, whereas the other patient had a retrievable OptEase filter that was not removed because the endarterectomy surgery was complicated by pulmonary bleeding and suspected heparin-induced thrombocytopenia. Because of the pulmonary history and the in situ IVC filter, therapeutic dose anticoagulants were prescribed to these patients. One patient had an IVC filter inserted for acute DVT at 30 weeks of gestation. She was treated with prophylactic dose with low-molecular-weight heparin (LMWH). The other IVC filters were inserted outside of pregnancy. All IVC filters were positioned infrarenally.
Amsterdam UMC cases: characteristics and outcomes for pregnancy in patients with in situ inferior vena cava filter
| Characteristics of patients at time of insertion IVC filter | Pregnancy characteristics and obstetric outcomes | Management and complications | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient no. | Age, y | Thrombotic history | Indication for filter and prepregnancy anticoagulant therapy | Location, type, and timing of filter insertion | Pregnancy no. | Years since IVC filter | Gravidity parity | Mode of delivery | Pregnancy outcome | LMWH dose during pregnancy | Pregnancy- related VTE?* | Complications† IVC filter |
| 1 | 31 | PE and mesenteric thrombosis | Surgery because of intra-abdominal bleeding 1 wk after acute PE DOAC (indefinite duration) | Infrarenal Retrievable (OptEase)‡ Outside pregnancy | 1 | 3 | G1P0 | Spontaneous vaginal delivery at 38w6d | Healthy neonate | Therapeutic | No | No |
| 2 | 21 | PE CTEPH, NYHA class II-III/IV | Pre-PEA VKA (indefinite duration) | Infrarenal Retrievable (OptEase)§ Outside pregnancy | 1 | 1 | G1P0 | Dilatation and curettage at <10 wk | Miscarriage | Therapeutic | No | No |
| 2 | 3 | G2P0 | Induced vaginal delivery at 41w6d | Healthy neonate | Therapeutic | No | No | |||||
| 3 | 5 | G3P1 | Induced vaginal delivery at 38w0d | Healthy neonate | Therapeutic | No | No | |||||
| 4 | 8 | G4P2 | Induced vaginal delivery at 38w4d | Healthy neonate | Therapeutic | No | No | |||||
| 3 | 29 | PE CTEPH, NYHA class III/IV | Pre-PEA VKA (indefinite duration) | Infrarenal Permanent (TrapEase) Outside pregnancy | 1 | 1 | G1P0 | Unknown, FU until 17 wk | Healthy neonate | Therapeutic | No | Noǁ |
| 4 | 27 | DVT | DVT in third trimester of pregnancy Low prophylactic LMWH since DVT diagnosis | Infrarenal Filter type unknown 30th week of pregnancy | 1 | 1 | G8P2 | Spontaneous vaginal delivery at 40w0d | Healthy neonate | Low prophylactic | Not during pregnancy | No |
| Characteristics of patients at time of insertion IVC filter | Pregnancy characteristics and obstetric outcomes | Management and complications | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient no. | Age, y | Thrombotic history | Indication for filter and prepregnancy anticoagulant therapy | Location, type, and timing of filter insertion | Pregnancy no. | Years since IVC filter | Gravidity parity | Mode of delivery | Pregnancy outcome | LMWH dose during pregnancy | Pregnancy- related VTE?* | Complications† IVC filter |
| 1 | 31 | PE and mesenteric thrombosis | Surgery because of intra-abdominal bleeding 1 wk after acute PE DOAC (indefinite duration) | Infrarenal Retrievable (OptEase)‡ Outside pregnancy | 1 | 3 | G1P0 | Spontaneous vaginal delivery at 38w6d | Healthy neonate | Therapeutic | No | No |
| 2 | 21 | PE CTEPH, NYHA class II-III/IV | Pre-PEA VKA (indefinite duration) | Infrarenal Retrievable (OptEase)§ Outside pregnancy | 1 | 1 | G1P0 | Dilatation and curettage at <10 wk | Miscarriage | Therapeutic | No | No |
| 2 | 3 | G2P0 | Induced vaginal delivery at 41w6d | Healthy neonate | Therapeutic | No | No | |||||
| 3 | 5 | G3P1 | Induced vaginal delivery at 38w0d | Healthy neonate | Therapeutic | No | No | |||||
| 4 | 8 | G4P2 | Induced vaginal delivery at 38w4d | Healthy neonate | Therapeutic | No | No | |||||
| 3 | 29 | PE CTEPH, NYHA class III/IV | Pre-PEA VKA (indefinite duration) | Infrarenal Permanent (TrapEase) Outside pregnancy | 1 | 1 | G1P0 | Unknown, FU until 17 wk | Healthy neonate | Therapeutic | No | Noǁ |
| 4 | 27 | DVT | DVT in third trimester of pregnancy Low prophylactic LMWH since DVT diagnosis | Infrarenal Filter type unknown 30th week of pregnancy | 1 | 1 | G8P2 | Spontaneous vaginal delivery at 40w0d | Healthy neonate | Low prophylactic | Not during pregnancy | No |
38w6d, 38 wk and 6 d of pregnancy; CTEPH, chronic thromboembolic pulmonary hypertension; DOAC: direct oral anticoagulant; FU, follow-up; G, gravidity; NYHA, New York Heart Association; P, parity; PEA, pulmonary endarterectomy; VKA: vitamin K antagonist.
During pregnancy or up to 6 wk postpartum.
Complications of IVC filter include: migration, tilt, fracture, penetration of the vena cava wall, IVC filter thrombosis, or bleeding caused by IVC filter complications.
Retrieval of IVC filter was attempted 4 wk after insertion and failed because the tip of the IVC filter was embedded in the endothelial wall. In an attempt to move the IVC filter, the IVC filter was slightly twisted. Retrieval remained impossible and the IVC filter was left in situ.
IVC filter was not removed after PEA surgery because this was complicated by a pulmonary bleeding and suspicion of heparin-induced thrombocytopenia
Radiologically confirmed: 6 mo before pregnancy, a venography showed an open IVC filter, 1 y after pregnancy abdominal x-ray showed an intact and correctly positioned IVC filter.
Among the 7 pregnancies in 4 patients, mean time since IVC filter insertion was 3.1 years (range, 1-8). One patient had 4 pregnancies. She had an early miscarriage followed by 3 induced term vaginal deliveries of healthy neonates. Other patients had 1 pregnancy. Two patients had uneventful pregnancies with term spontaneous deliveries of healthy neonates. For the fourth patient, details were only available up to 17 weeks of gestation and she gave birth to a healthy neonate. Mean gestational age at delivery was 39 weeks and 5 days (range, 38 weeks 0 days-41 weeks 6 days) (Table 1). The mode of delivery was based on obstetric indications in all cases.
The first pregnancy after IVC filter insertion was unplanned in 3 patients and occurred before patients had been counseled about the risks of an in situ IVC filter during pregnancy. Filter integrity prior to pregnancy was not assessed in 4 (57%) pregnancies. In 1 (14%) pregnancy, the presence of an open and intact IVC filter was confirmed by ultrasound examination during the first trimester. In 2 (29%) pregnancies, imaging with compression ultrasound or venography was performed 6 months before conception to exclude acute thrombosis and revealed open IVC filters. In 1 (14%) of these pregnancies, imaging of the IVC filter was also performed after pregnancy and revealed no IVC filter complications. In 6 (86%) other pregnancies, although not radiologically confirmed, no signs or symptoms of migration, tilt, fracture, penetration of vena cava wall, IVC filter thrombosis, or bleeding caused by IVC filter complications occurred. Concomitant anticoagulant therapy with LMWH was prescribed in all pregnancies: therapeutically dosed in 6 (86%) pregnancies in patients who were on therapeutic dose anticoagulants before their pregnancies, and low prophylactic dose in 1 pregnancy in the patient who was on prophylactic dose LMWH since her DVT diagnosis. No pregnancy-related recurrent VTE was observed (Table 1).
Literature review
The literature search yielded 156 unique articles and 4 abstracts (Figure 2). After screening of title and abstract, 105 records were excluded. Fifty-five full-text articles were assessed: 16 were excluded because the study population did not meet the target population, 24 articles were excluded because data on IVC filter retrieval and/or subsequent pregnancy were not provided, and for 10 records full-text was not available. We included 1 retrospective cohort study, 2 case series on IVC filter use in pregnancy (containing data on both peripartum use of IVC filter and pregnancies with in situ IVC filter before conception), and 2 case reports (supplemental Table 2). Rottenstreich et al9 presented a cohort of 24 cases who underwent retrievable IVC filter placement during pregnancy or in the postpartum period; only 1 patient had subsequent pregnancies with an IVC filter still in situ. Gupta et al16 presented 12 pregnancies in 6 women with retrievable and permanent IVC filters, of which 8 pregnancies occurred in 5 patients after the IVC filter had been inserted. Thomas et al17 described the use of Greenfield filters in 8 pregnant patients, of whom 1 became pregnant after IVC filter placement. Maijub et al18 presented a case of uterine trauma with fetal loss associated with chronic perforation of the inferior vena cava by an IVC filter. Lee et al19 reported a young woman with recurrent VTE due to antiphospholipid syndrome who became pregnant with an in situ IVC filter. Quality assessment of the studies is summarized in supplemental Table 3. Information on IVC filter complications and pregnancy outcome was poorly described by Rottenstreich et al9 and Lee et al.19 In the latter, only information on VTE recurrence was provided.
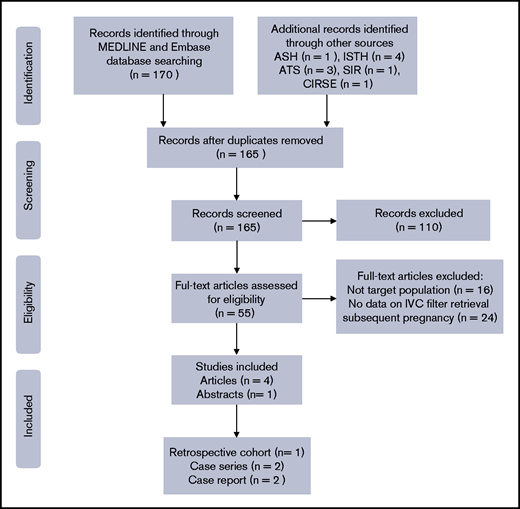
PRISMA flow diagram of literature search. ASH, American Society of Hematology; ATS, American Thoracic Society; CIRSE, Cardiovascular and Interventional Radiological Society of Europe; ISTH, International Society on Thrombosis and Haemostasis; SIR, Society of Interventional Radiology.
PRISMA flow diagram of literature search. ASH, American Society of Hematology; ATS, American Thoracic Society; CIRSE, Cardiovascular and Interventional Radiological Society of Europe; ISTH, International Society on Thrombosis and Haemostasis; SIR, Society of Interventional Radiology.
In all studies combined, we collected data of 13 pregnancies in 9 patients with an in situ IVC filter before conception. Patient and pregnancy characteristics as well as outcomes are listed in Table 2. The mean age at IVC filter insertion was 26.3 years (range, 17-35) and indication was VTE in all cases. Three (33%) patients had a retrievable IVC filter (among others, Günther Tulip) that remained in situ after failed retrieval, 5 (56%) patients had a permanent IVC filter (Bird’s Nest, Greenfield, TrapEase), and IVC filter type was not reported for 1 patient. Five (56%) IVC filters were inserted outside of pregnancy and 4 (44%) IVC filters during a previous pregnancy. Four (44%) patients were nulliparous at time of IVC filter insertion. Two patients had been diagnosed with preexistent complications of the IVC filter: 1 patient had IVC filter misplacement into the external iliac vein with penetration of the inferior vena cava wall9 and 1 patient was diagnosed with asymptomatic chronic perforation of the inferior vena cava by struts and barbs of the IVC filter.18
Literature reviews: characteristics and outcomes for pregnancy in patients with in situ inferior vena cava filter
| Characteristics at time of insertion IVC filter | Pregnancy characteristics and obstetric outcomes | Management and complications | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient no., study | Age, y | Indication | Location, type, and timing | Pregnancy no. | Years since IVC filter | Parity | Mode of delivery | Pregnancy outcome | Anticoagulants during pregnancy | Pregnancy- related VTE?* | Complications† IVC filter |
| 19 | 32 | PE | Infrarenal Retrievable (subtype NR)‡ 15th week of pregnancy | 1 | NR | NR | NR | “Uneventful pregnancy” | LMWH ± ASA§ | NR | NR |
| 2 | NR | NR | NR | “Uneventful pregnancy” | LMWH ± ASA§ | NR | NR | ||||
| 216 | 17 | PE following recent surgery | Location NR Retrievable (Günther Tulip)ǁ Outside pregnancy | 1 | 3 | 0 | Emergency CS at 42 wk | Healthy neonate | ASA | No | No |
| 2 | 5 | 1 | Elective CS at 40 wk | Healthy neonate | ASA | No | No | ||||
| 3 | 7 | 2 | Elective CS at 38 wk | Healthy neonate | ASA | No | No | ||||
| 316 | 27 | Recurrent VTE despite anticoagulants | Location NR Permanent (Bird’s Nest) Outside pregnancy | 1 | 2 | 0 | Spontaneous vaginal delivery at 39 wk | Healthy neonate | LMWH¶ | No | No |
| 2 | 4 | 1 | Spontaneous vaginal delivery at 38 wk | Healthy neonates (twins) | LMWH¶ | No | No | ||||
| 416 | 35 | Pregnancy-related DVT | Location NR Permanent (Bird’s Nest) 35th week of pregnancy | 1 | 4 | 1 | Spontaneous vaginal delivery at 41 wk | Healthy neonate | LMWH¶ | No | No |
| 516 | 23 | Pregnancy-related DVT | Location NR Permanent (Bird’s Nest) 11th week of pregnancy | 1 | 8 | 1 | Elective CS at 38 wk | Healthy neonate | LMWH¶ | No | No |
| 616 | 25 | Pregnancy-related DVT | Location NR Retrievable (Günther Tulip)ǁ 34th week of pregnancy | 1 | 4 | 1 | Emergency CS at 41 wk | Healthy neonate | LMWH¶ | No | No |
| 717 | 24 | DVT | Location NR Permanent (Greenfield) Outside pregnancy | 1 | NR | 1 | Spontaneous vaginal delivery at 36 wk | Healthy neonate | NR | No | No |
| 818 | 27 | Recurrent VTE, warfarin allergy, and retroperitoneal hematoma | Infrarenal Permanent (TrapEase)# Outside pregnancy | 1 | 4 | 0 | Emergency CS at 24 wk | Fetus died shortly after birth | LMWH¶ | No | Uterine trauma and massive intraperitoneal hemorrhage caused by perforation of IVC filter struts |
| 919 | 27 | Recurrent VTE | Location and filter type NR Outside pregnancy | 1 | <1 | 0 | NR | NR | LMWH¶ | No | NR |
| Characteristics at time of insertion IVC filter | Pregnancy characteristics and obstetric outcomes | Management and complications | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient no., study | Age, y | Indication | Location, type, and timing | Pregnancy no. | Years since IVC filter | Parity | Mode of delivery | Pregnancy outcome | Anticoagulants during pregnancy | Pregnancy- related VTE?* | Complications† IVC filter |
| 19 | 32 | PE | Infrarenal Retrievable (subtype NR)‡ 15th week of pregnancy | 1 | NR | NR | NR | “Uneventful pregnancy” | LMWH ± ASA§ | NR | NR |
| 2 | NR | NR | NR | “Uneventful pregnancy” | LMWH ± ASA§ | NR | NR | ||||
| 216 | 17 | PE following recent surgery | Location NR Retrievable (Günther Tulip)ǁ Outside pregnancy | 1 | 3 | 0 | Emergency CS at 42 wk | Healthy neonate | ASA | No | No |
| 2 | 5 | 1 | Elective CS at 40 wk | Healthy neonate | ASA | No | No | ||||
| 3 | 7 | 2 | Elective CS at 38 wk | Healthy neonate | ASA | No | No | ||||
| 316 | 27 | Recurrent VTE despite anticoagulants | Location NR Permanent (Bird’s Nest) Outside pregnancy | 1 | 2 | 0 | Spontaneous vaginal delivery at 39 wk | Healthy neonate | LMWH¶ | No | No |
| 2 | 4 | 1 | Spontaneous vaginal delivery at 38 wk | Healthy neonates (twins) | LMWH¶ | No | No | ||||
| 416 | 35 | Pregnancy-related DVT | Location NR Permanent (Bird’s Nest) 35th week of pregnancy | 1 | 4 | 1 | Spontaneous vaginal delivery at 41 wk | Healthy neonate | LMWH¶ | No | No |
| 516 | 23 | Pregnancy-related DVT | Location NR Permanent (Bird’s Nest) 11th week of pregnancy | 1 | 8 | 1 | Elective CS at 38 wk | Healthy neonate | LMWH¶ | No | No |
| 616 | 25 | Pregnancy-related DVT | Location NR Retrievable (Günther Tulip)ǁ 34th week of pregnancy | 1 | 4 | 1 | Emergency CS at 41 wk | Healthy neonate | LMWH¶ | No | No |
| 717 | 24 | DVT | Location NR Permanent (Greenfield) Outside pregnancy | 1 | NR | 1 | Spontaneous vaginal delivery at 36 wk | Healthy neonate | NR | No | No |
| 818 | 27 | Recurrent VTE, warfarin allergy, and retroperitoneal hematoma | Infrarenal Permanent (TrapEase)# Outside pregnancy | 1 | 4 | 0 | Emergency CS at 24 wk | Fetus died shortly after birth | LMWH¶ | No | Uterine trauma and massive intraperitoneal hemorrhage caused by perforation of IVC filter struts |
| 919 | 27 | Recurrent VTE | Location and filter type NR Outside pregnancy | 1 | <1 | 0 | NR | NR | LMWH¶ | No | NR |
ASA, acetylsalicylic acid; CS, cesarean section; NR, not reported.
During pregnancy or up to 6 wk postpartum.
Complications of IVC filter include: migration, tilt, fracture, penetration of the vena cava wall, IVC filter thrombosis, or bleeding caused by IVC filter complications.
Complicated insertion: filter misplacement into external iliac vein, associated penetration of IVC wall.
It was unclear whether ASA was added to LMWH treatment in this pregnancy.
Failure of IVC retrieval.
Dose of LMWH was not reported
Known complication IVC filter before pregnancy: asymptomatic, chronic perforation of the IVC wall by struts and barbs of the IVC filter.
The mean time since IVC filter insertion at time of pregnancy was 4.2 years (range, <1-8). One patient had 3 pregnancies with in situ IVC filter, 2 patients had 2 pregnancies and 6 patients had 1 pregnancy. The mode of delivery was spontaneous vaginal delivery in 4 (31%) pregnancies, cesarean section in 6 (46%) pregnancies (3 emergency, 3 elective), and was not reported in 3 (23%) pregnancies. The patient with 3 pregnancies had an emergency cesarean section at first delivery and gave birth to her following 2 babies through elective cesarean section. Mean gestational age at delivery was 37 weeks and 5 days (range, 24-42). One (8%) patient had a twin pregnancy and pregnancy outcome was not reported for 1 patient. Twelve (86%) healthy neonates were born, 1 (8%) pregnancy was complicated by IVC filter perforation that resulted in emergency cesarean section at 24 weeks and 2 days of pregnancy.18 The fetus died shortly after birth. Perforating barbs and struts of the permanent TrapEase filter caused uterine lacerations and a tear in the peritoneal membrane, leading to major intra-abdominal hemorrhage. In 1 (8%) pregnancy, outcomes were not reported, whereas the other 11 (85%) pregnancies were uneventful. Concomitant antithrombotic therapy was administered and consisted of acetylsalicylic acid monotherapy in 3 (23%) pregnancies, unspecified doses of LMWH in nine (69%) pregnancies and was not reported in 1 pregnancy. No pregnancy-related VTE were reported (Table 2).
An overview of characteristics and appearances of the IVC filters mentioned in this section can be found in Table 3.

Discussion
In this study, we compiled results on risk of complications of in situ IVC filters in 7 pregnancies in 4 patients from our tertiary center and in 13 pregnancies in 9 patients derived from an extensive and systematic literature search. In 1 pregnancy, described as a single case report, uterine trauma with fetal loss was observed. Other pregnancies were uneventful. Because of the low number of only 20 identified pregnancies, and the intrinsic biases of this type of publications, we are unable to draw firm conclusions with regard to safety of in situ IVC filter during pregnancy. Importantly, the patient who had a severe complication was known to have pre-existent perforation of the vena cava wall before her pregnancy, which was asymptomatic until pregnancy progressed. Therefore, we would suggest performing imaging of the IVC filter to exclude asymptomatic IVC filter complications in all women contemplating pregnancy. In a study on perforations by IVC filters in 391 patients, 69% perforations were isolated IVC wall perforations and roughly one-half of the patients were asymptomatic.20 The aorta, duodenum, and vertebral bodies were the most frequently perforated surrounding organs.20 IVC perforation should ideally be excluded using computed tomography or venography.2 Thrombotic occlusion, tilt fracture, or embolization of the IVC filter could also be detected using conventional radiography and ultrasonography.2
Filters that were inserted during pregnancy have been previously reported to be able to cause symptomatic perforation of the uterus21 and cephalic migration into the right atrium22 within hours to days after insertion. Moreover, asymptomatic IVC filter fracture and migration was detected up to 5 months postpartum when attempting to retrieve the IVC filter.23‐25 If the IVC filter has been in situ for some time, one might postulate that it is less likely to migrate because of endothelialization. The IVC filters inserted during pregnancy in the presently described cases did not lead to complications shortly after insertion, which could be a predictor for favorable outcome during a subsequent pregnancy. In general, the risk of migration of IVC filter during pregnancy seems to be increased because of dilatation and the risk of fracture from change in IVC configuration.26
Following the 2010 Food and Drug Administration safety alert on the risks of permanent indwelling of retrievable IVC filters,12 there has been a notable decline in insertions of IVC filters.27,28 Routine insertion of IVC filters before pulmonary endarterectomy was initially recommended,29 but this practice is no longer supported by the current guideline of the European Society of Cardiology and European Respiratory Society.30 Additionally, data from an international prospective registry on patients with chronic thromboembolic pulmonary hypertension showed that the presence of an IVC filter in 40% of patients did not influence long-term survival.31 Although the use of IVC filters has declined, given the failure rate of retrieval, the clinical issue of young women with an in situ IVC filter contemplating pregnancy is still a reality.
The obvious limitation of this study is the small number of patients in our cohort as well as scarcity of published data on the course of pregnancy in women with an in situ IVC filter. The literature search is at risk for publication bias, particularly for case reports, where complicated cases might overestimate the risk of IVC filter complications. Strengths are the complete collection of data from our own center, as well as the published literature.
Conclusion
In conclusion, based on a tertiary center case series and literature search, we report a serious IVC filter complication in 1 of 20 pregnancies. The single complication described during pregnancy was in an asymptomatic patient who had a perforated IVC filter in situ before conception. Therefore, it seems safe to become pregnant with an indwelling IVC filter that is intact and does not show signs of perforation, but because of the low number of cases, no firm conclusions about safety of permanent IVC filters during pregnancy can be drawn. We suggest imaging, preferably before pregnancy, to reveal asymptomatic IVC filter complications.
Authorship
Contribution: I.M.B. designed the study, reviewed medical charts, collected data, performed literature search and data extraction, and wrote the first draft of the manuscript; A.E.G. performed literature search and data extraction and critically reviewed and revised the manuscript; P.I.B., W.G., and I.A.J.Z. critically reviewed and revised the manuscript; S.M. designed the study and critically reviewed and revised the manuscript; and all authors approved the final version of the manuscript.
Conflict-of-interest disclosure: No funding was obtained for this study and the authors declare no competing financial interests. The authors report the following unrelated support: S.M. reports grants and personal fees from Daiichy Sankyo, Bayer, Pfizer, and Boehringer-Ingelheim; and personal fees from Portola, Abbvie, and BMS Pfizer. W.G. reports in-kind contribution of study materials from Roche Diagnostics for investigator-initiated studies.
Data sharing statement: For original data, please contact i.m.bistervels@amsterdamumc.nl.
Correspondence: Ingrid Bistervels, Amsterdam UMC, University of Amsterdam, Department of Vascular Medicine, Amsterdam Cardiovascular Sciences, Meibergdreef 9, 1105 AZ Amsterdam, The Netherlands; e-mail: i.m.bistervels@amsterdamumc.nl.

