

Key Points
Treatment-naive and relapsed/refractory MDS patients receiving venetoclax and HMAs have an ORR of 59% with 63% of responders proceeding to transplant.
Allogeneic stem cell transplantation after treatment with venetoclax in combination with HMA is associated with prolonged survival.

Introduction
Hypomethylating agents (HMAs) are the current standard of care in high-risk myelodysplastic syndromes (MDS). However, only ∼50% of patients with MDS respond to HMAs and most responding patients eventually progress.1,2 Outcomes after HMA failure are particularly poor, with a median overall survival (OS) of 4 to 6 months.3,4 Venetoclax is an oral selective inhibitor of the anti-apoptotic protein BCL-2 and, in combination with azacitidine, increased responses and prolonged survival when compared with azacitidine alone in a phase 3 study for patients with previously-untreated acute myeloid leukemia (AML), ineligible for intensive chemotherapy.5 Preclinical studies have demonstrated that BCL-2 is overexpressed in high-risk MDS, and BCL-2 inhibition induces apoptosis in MDS progenitor cells.6,7 However, MDS is defined by bone marrow dysplasia and cytopenias, and the addition of venetoclax to HMAs in MDS has potential for cumulative myelosuppression. Phase 1 studies evaluating venetoclax in combination with HMAs in treatment-naïve and relapsed/refractory (R/R) MDS are currently under investigation.8,9 Here, we present real-world evidence supporting the use of venetoclax in combination with HMAs in patients with MDS. We also identify risk factors impacting response and survival after treatment with the combination.
Patients and methods
Medical records of 44 patients with MDS receiving venetoclax in combination with HMAs at Memorial Sloan Kettering Cancer Center (MSKCC) (n = 11), Moffitt Cancer Center (n = 23), University of Pennsylvania (n = 5), Hackensack University Medical Center (n = 2), and Yale University (n = 3) between January 2018 and July 2019 were reviewed. This study was approved by the MSKCC institutional review board. Criteria for inclusion were a pathologically confirmed diagnosis of MDS,10 age >18 years, and ≥1 cycle of decitabine or azacitidine in combination with venetoclax. Venetoclax was prescribed off-label and dependent on insurance approval. HMA-naïve patients and patients previously treated with HMAs were included. Patients with a diagnosis other than MDS or progression to AML before treatment with HMA + venetoclax were excluded. HMA failure was defined as a lack of response after 4 cycles of HMA, progressive disease after at least 2 cycles of HMA, or progressive disease after achieving a response. Responses were evaluated per the International Working Group criteria.11 Hematology values for up to 2 weeks after bone marrow evaluation were used to determine response. Pretreatment cytogenetics and next-generation sequencing were performed per institutional standards, and, when available, included for analysis.
Patient characteristics were summarized by frequency (percentage). Associations between overall response and patient and disease characteristics were tested by Fisher's exact test. OS and relapse-free survival (RFS) were evaluated by the Kaplan-Meier method, and the difference between groups was determined by log-rank test. The effects of patient and disease characteristics on OS were estimated by the univariate Cox proportional hazard model, with P < .05 being considered significant. All statistical analyses were performed using R.
Results and discussion
Baseline patient characteristics are reported in Table 1. Predominant features of the patient cohort included Revised International Prognostic Scoring System (IPSS-R) very high-risk (41%), poor or very poor-risk cytogenetics (43%), prior treatment with HMA (73%), and >10% blasts on pretreatment bone marrow biopsy (57%). TP53 mutations with complex karyotype occurred in 28% of patients with available sequencing data (supplemental Figure 1). In combination with venetoclax, 61% received azacitidine 75 mg/m2 for 7 days and 39% received decitabine 20 mg/m2 for 5 days. Treatment with decitabine was overrepresented among patients with TP53 mutations (64% vs 36%, P = .07). The starting dose of venetoclax was 400 mg (42%), 200 mg (37%), and ≤100 mg (21%) with dose adjustment for use of azole antifungals. Duration of venetoclax during the first cycle was 14 days (9%), 21 days (14%), and 28 days (77%).
Characteristics and univariate analysis of factors associated with response and survival of the 44 MDS patients who received venetoclax and hypomethylating agent therapy
| Baseline characteristics | Overall response, % | Overall survival | |||||
|---|---|---|---|---|---|---|---|
| Variable | Total evaluable, n | Frequency, n (%) | Yes | No | P | HR (95% CI) | Log rank |
| Age, y | 44 | .13 | 0.10 | ||||
| ≤60 | 8 (18) | 62 | 38 | 1 | |||
| 60-67 | 11 (25) | 82 | 18 | 1.76 (0.16-19.51) | |||
| 67-74 | 13 (30) | 62 | 38 | 4.47 (0.54-37.28) | |||
| >74 | 12 (27) | 33 | 67 | 6.64 (0.83-53.36) | |||
| Sex | 44 | .36 | 0.16 | ||||
| Male | 24 (55) | 67 | 33 | 1 | |||
| Female | 20 (45) | 50 | 50 | 2.00 (0.75-5.33) | |||
| Therapy related | 44 | .11 | <0.01 | ||||
| No | 29 (66) | 69 | 31 | 1 | |||
| Yes | 15 (34) | 40 | 60 | 3.82 (1.4-10.46) | |||
| HMA exposure | 44 | .26 | 0.82 | ||||
| Naive | 12 (28) | 75 | 25 | 1 | |||
| ≤4 cycles | 16 (36) | 62 | 38 | 1.12 (0.30-4.2) | |||
| HMA failure | 16 (36) | 44 | 56 | 1.43 (0.42-4.84) | |||
| Bone marrow blast, T0, % | 44 | .54 | 0.30 | ||||
| >10 | 25 (57) | 64 | 36 | 1 | |||
| ≤10 | 19 (43) | 53 | 47 | 1.64 (0.63-4.26) | |||
| R-IPSS cytogenetic risk | 43 | .03 | <0.01* | ||||
| Other | 33 (77) | 70 | 30 | 1 | |||
| Very poor risk | 10 (23) | 30 | 70 | 9.21 (3.04-27.89) | |||
| TP53 mutated | 40 | .15 | <0.01* | ||||
| No | 29 (72) | 66 | 34 | 1 | |||
| Yes | 11 (28) | 36 | 64 | 8.32 (2.48-27.96) | |||
| R-IPSS risk | 42 | .12 | <0.01* | ||||
| Other | 24 (57) | 71 | 29 | 1 | |||
| Very high risk | 18 (43) | 44 | 56 | 7.94 (2.2-28.68) | |||
| Type of HMA with venetoclax | 44 | .22 | 0.03 | ||||
| Azacitidine | 27 (61) | 67 | 33 | 1 | |||
| Decitabine | 17 (39) | 47 | 53 | 2.78 (1.05-7.35) | |||
| Venetoclax dose, T0, mg | 43 | 1 | 0.45 | ||||
| 400 | 18 (42) | 61 | 39 | 1 | |||
| 200 | 16 (37) | 62 | 38 | 0.81 (0.23-2.81) | |||
| ≤100 | 9 (21) | 56 | 44 | 1.78 (0.56-5.65) | |||
| Azole antifungals | 44 | .36 | 0.39 | ||||
| No | 25 (57) | 52 | 48 | 1 | |||
| Yes | 19 (43) | 68 | 32 | 1.53 (0.58-4.01) | |||
| Cycle 2 or 3 delay ≥7 d | 24 | .41 | 0.92 | ||||
| No | 8 (33) | 50 | 50 | 1.09 (0.21-5.56) | |||
| Yes | 16 (67) | 69 | 31 | 1 | |||
| Venetoclax dosing first cycle, d | 44 | .42 | 0.56 | ||||
| ≤14 | 4 (9) | 50 | 50 | 1 | |||
| 15-21 | 6 (14) | 83 | 17 | 0.51 (0.13-1.69) | |||
| 22-28 | 34 (77) | 56 | 44 | 0.47 (0.10-2.71) | |||
| Baseline characteristics | Overall response, % | Overall survival | |||||
|---|---|---|---|---|---|---|---|
| Variable | Total evaluable, n | Frequency, n (%) | Yes | No | P | HR (95% CI) | Log rank |
| Age, y | 44 | .13 | 0.10 | ||||
| ≤60 | 8 (18) | 62 | 38 | 1 | |||
| 60-67 | 11 (25) | 82 | 18 | 1.76 (0.16-19.51) | |||
| 67-74 | 13 (30) | 62 | 38 | 4.47 (0.54-37.28) | |||
| >74 | 12 (27) | 33 | 67 | 6.64 (0.83-53.36) | |||
| Sex | 44 | .36 | 0.16 | ||||
| Male | 24 (55) | 67 | 33 | 1 | |||
| Female | 20 (45) | 50 | 50 | 2.00 (0.75-5.33) | |||
| Therapy related | 44 | .11 | <0.01 | ||||
| No | 29 (66) | 69 | 31 | 1 | |||
| Yes | 15 (34) | 40 | 60 | 3.82 (1.4-10.46) | |||
| HMA exposure | 44 | .26 | 0.82 | ||||
| Naive | 12 (28) | 75 | 25 | 1 | |||
| ≤4 cycles | 16 (36) | 62 | 38 | 1.12 (0.30-4.2) | |||
| HMA failure | 16 (36) | 44 | 56 | 1.43 (0.42-4.84) | |||
| Bone marrow blast, T0, % | 44 | .54 | 0.30 | ||||
| >10 | 25 (57) | 64 | 36 | 1 | |||
| ≤10 | 19 (43) | 53 | 47 | 1.64 (0.63-4.26) | |||
| R-IPSS cytogenetic risk | 43 | .03 | <0.01* | ||||
| Other | 33 (77) | 70 | 30 | 1 | |||
| Very poor risk | 10 (23) | 30 | 70 | 9.21 (3.04-27.89) | |||
| TP53 mutated | 40 | .15 | <0.01* | ||||
| No | 29 (72) | 66 | 34 | 1 | |||
| Yes | 11 (28) | 36 | 64 | 8.32 (2.48-27.96) | |||
| R-IPSS risk | 42 | .12 | <0.01* | ||||
| Other | 24 (57) | 71 | 29 | 1 | |||
| Very high risk | 18 (43) | 44 | 56 | 7.94 (2.2-28.68) | |||
| Type of HMA with venetoclax | 44 | .22 | 0.03 | ||||
| Azacitidine | 27 (61) | 67 | 33 | 1 | |||
| Decitabine | 17 (39) | 47 | 53 | 2.78 (1.05-7.35) | |||
| Venetoclax dose, T0, mg | 43 | 1 | 0.45 | ||||
| 400 | 18 (42) | 61 | 39 | 1 | |||
| 200 | 16 (37) | 62 | 38 | 0.81 (0.23-2.81) | |||
| ≤100 | 9 (21) | 56 | 44 | 1.78 (0.56-5.65) | |||
| Azole antifungals | 44 | .36 | 0.39 | ||||
| No | 25 (57) | 52 | 48 | 1 | |||
| Yes | 19 (43) | 68 | 32 | 1.53 (0.58-4.01) | |||
| Cycle 2 or 3 delay ≥7 d | 24 | .41 | 0.92 | ||||
| No | 8 (33) | 50 | 50 | 1.09 (0.21-5.56) | |||
| Yes | 16 (67) | 69 | 31 | 1 | |||
| Venetoclax dosing first cycle, d | 44 | .42 | 0.56 | ||||
| ≤14 | 4 (9) | 50 | 50 | 1 | |||
| 15-21 | 6 (14) | 83 | 17 | 0.51 (0.13-1.69) | |||
| 22-28 | 34 (77) | 56 | 44 | 0.47 (0.10-2.71) | |||
Boldface numbers indicate variables with P < .05.
CI, confidence interval; T0, time at start of combination treatment.
P values below Bonferroni-adjusted level considering all comparisons, 0.0017 (0.05/30).
During the first cycle of treatment, none of the patients experienced clinical tumor lysis syndrome (supplemental Table 1). A delay (>7 days) in initiation of cycle 2 or 3 and an interruption (>7 days) of venetoclax dosing occurred in 67% and 29% of patients, respectively. Hospitalization for any cause other than tumor lysis syndrome monitoring occurred in 32% of patients. Combination treatment was discontinued because of adverse events in 20% of patients, including anemia (n = 1), thrombocytopenia (n = 1), neutropenia (n = 2), neutropenic fevers (n = 4), and unknown (n = 1). Death within the first 30, 60, and 90 days occurred in 5% (n = 2), 11% (n = 5), and 11% (n = 5) of patients, respectively (supplemental Table 2).
For the total cohort, the overall response was 59%, including 14% with a complete response (CR), 27% with a marrow CR with hematologic improvement (HI), and 18% with a marrow CR without HI. Median time to initial response was 1.6 months (range, 1-3 months). Of 8 patients at MSKCC who underwent multiparameter flow cytometry according to previously published methods,12 2 (25%) had no immunophenotypic evidence of disease (supplemental Table 4). On univariate analysis, very poor-risk cytogenetics by IPSS-R was the only factor associated with a significant decrease in overall response (Table 1). HMA exposure did not affect response (Figure 1A; Table 1).
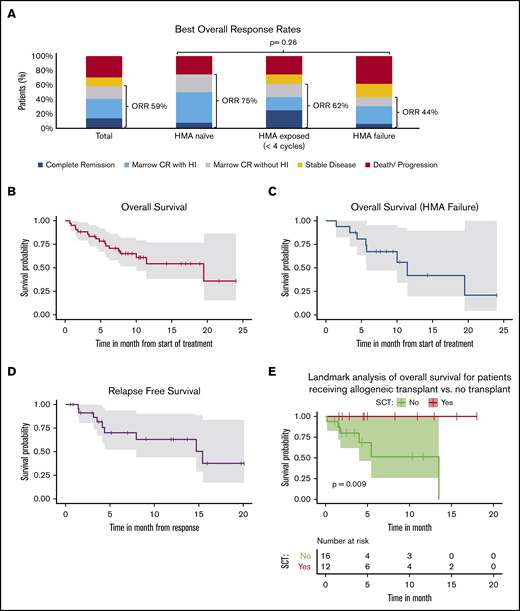
Response and survival of patients with myelodysplastic syndrome (MDS) receiving venetoclax in combination with hypomethylating agent therapy. (A) Best overall response rate was 59% for the entire cohort and not significantly different by HMA exposure (ORR: HMA naïve 75%, HMA ≤4 cycles 62%, and HMA failure 44%, P = .26). (B) Kaplan-Meier (KM) curve of OS for the entire cohort. The median OS was 19.5 months (95% CI, 10.0 to not estimable). (C) KM curve of OS for patients with HMA failure before starting venetoclax + HMA. The median OS was 11.4 months (95% CI, 5.7 to not estimable). (D) KM curve of relapse-free survival (RFS) for the entire cohort. The median RFS was 15.4 months (95% CI, 7.9 to not estimable). (E) Landmark analysis at 6 months after starting treatment with venetoclax and HMA demonstrating significantly longer survival (P = .009) for patients with MDS undergoing allogeneic transplant (SCT: yes) when compared with those not undergoing transplant (SCT: no). Only patients surviving at 6 months were included in the analysis.
Response and survival of patients with myelodysplastic syndrome (MDS) receiving venetoclax in combination with hypomethylating agent therapy. (A) Best overall response rate was 59% for the entire cohort and not significantly different by HMA exposure (ORR: HMA naïve 75%, HMA ≤4 cycles 62%, and HMA failure 44%, P = .26). (B) Kaplan-Meier (KM) curve of OS for the entire cohort. The median OS was 19.5 months (95% CI, 10.0 to not estimable). (C) KM curve of OS for patients with HMA failure before starting venetoclax + HMA. The median OS was 11.4 months (95% CI, 5.7 to not estimable). (D) KM curve of relapse-free survival (RFS) for the entire cohort. The median RFS was 15.4 months (95% CI, 7.9 to not estimable). (E) Landmark analysis at 6 months after starting treatment with venetoclax and HMA demonstrating significantly longer survival (P = .009) for patients with MDS undergoing allogeneic transplant (SCT: yes) when compared with those not undergoing transplant (SCT: no). Only patients surviving at 6 months were included in the analysis.
At the time of data cutoff, 17 (39%) patients had died and 27 (61%) were alive. With a median follow-up of 7.6 months (range, 0.3-23.6) after treatment initiation, the median OS was 19.5 months (95% CI, 10.0 to not estimable) for the entire cohort and 11.4 months (95% CI, 5.7 to not estimable) among patients with HMA failure (Figure 1B-C). Median RFS was 15.4 months (95% CI, 7.9 to not estimable) (Figure 1D). Factors affecting OS on univariate analysis included therapy-related neoplasm (T-MN), IPSS-R very high-risk, very poor-risk cytogenetics, the presence of a TP53 mutation, and treatment with decitabine (Table 1). Very poor-risk cytogenetics, T-MN, and the presence of a TP53 mutation were not confounded by center based on our stratified analysis (supplemental Table 4). Additionally, decitabine did not significantly affect survival after adjusting for TP53 mutation status (hazard ratio, 1.6; P = .38). Allogeneic stem cell transplantation (alloSCT) was performed in 16 of 26 (62%) patients achieving response. Landmark at 6 months and time-dependent covariate analyses demonstrated that patients receiving alloSCT had significantly longer median OS (hazard ratio, 0.1; 95% CI, 0.01-0.82) (Figure 1E).
Here, we report that venetoclax in combination with HMA led to high rates of marrow remission (59%) and HI (41%) in a heavily pretreated and high-risk MDS population. We observed similar response rates among HMA-naïve and HMA-failure patients when compared with the phase 1b clinical trials of venetoclax and HMA in treatment-naïve (overall response rate [ORR], 77%)9 and R/R (ORR, 40%)8 MDS. Treatment with the combination also led to high rates of alloSCT in 62% of all responding patients, which is notable because alloSCT was associated with prolonged survival. We also identified factors associated with decreased survival including very poor-risk cytogenetics, T-MN, and the presence of a TP53 mutation. The poor OS for those with TP53 mutations and complex karyotypes receiving venetoclax and HMA is consistent with reports in AML.13,14 We observed higher rates of treatment discontinuation because of adverse events (21%) than in newly diagnosed or R/R AML, suggesting increased myelosuppression in MDS.13,15 Of note, starting venetoclax dose and dose reductions did not affect response or survival in our analysis. However, our study was retrospective and limited by the small patient numbers, heterogeneous patient population, and short follow-up. We recommend following ongoing clinical trials for guidance on the dosing and schedule of venetoclax and HMA. In the phase 1b study of patients with treatment-naïve MDS, the recommended phase 2 dose of venetoclax was 400 mg for days 1 through 14 of a 28-day cycle when combined with azacitidine.9 Last, venetoclax and HMA led to response in 44% and a median OS of 11.4 months in patients with HMA failure. This compares favorably to the median OS of 4 to 6 months that has previously been reported for this population.3,4 Our retrospective real-world data suggest that adding venetoclax may salvage patients failing to respond optimally to HMA, thus allowing more patients to proceed to alloSCT. We await the results of phase 3 studies to definitively address whether adding venetoclax to azacitidine provides benefit in high-risk MDS.
Data sharing requests can be e-mailed to the corresponding author, Aaron D. Goldberg (goldbera@mskcc.org).
Acknowledgment
The authors thank all of the physicians and medical staff of the participating centers that took care of the patients and helped to collect data.
Authorship
Contribution: B.J.B., A.D.G., and R.S.K. contributed equally to conceiving and designing the study, collecting and interpreting data, and writing the manuscript; A.D. performed the statistical analysis and analyzed and interpreted data; and all authors performed research, collected data, and wrote and approved the manuscript.
Conflict-of-interest disclosure: E.M.S. served on the board of directors or advisory committee for Agios, Astellas Pharma US, Celgene, Daiichi Sankyo, Genentech, Novartis, PTC Therapeutics, Syros, Bioline, and Biotheryx and served as a consultant for Agios. M.S.T. receives research funding from ADC Therapeutics, Biosight, AbbVie, Cellerant, Orsenix, Glycomimetics, Rafael, and Amgen; served on the advisory board for Rigel, Nohla, BioLineRx, Oncolyze, Δ Fly Pharma, Daiichi-Sankyo, KAHR, AbbVie, Orsenix, Tetraphase, Jazz, and Roche; and receives royalties from UpToDate. S.I.G. received research funding from Novartis, Tmunity Therapeutics, and Carisma Therapeutics; served on advisory panel/consultant for Amphivena, Aro, Intellia, and Sensei Bio; and has equity ownership in Carisma Therapeutics. J.K. served on speakers bureau for Amgen, AbbVie, and Novartis and received honoraria from Pfizer. T.P. received research funding from Jazz, BMS, and Agios and honoraria from Genentech, Agios, Pfizer, and Novartis. E.P. received research funding from Incyte, Kura Oncology, Celgene. D.A.S. served on speaker’s bureaus for Novartis, AbbVie, Incyte, and Celgene; received research funding from Celgene and Jazz; and served on a board of directors or advisory committee for Celyad. R.S.K. served as a consultant for Pfizer, DSI, Incyte, Agios, Celgene, Jazz and served on a speaker’s bureau for Novartis and Jazz. A.D.G. served on advisory boards or as a consultant for AbbVie, Aptose, Celgene, Daiichi Sankyo, and Genentech; received research funding from AbbVie, ADC Therapeutics, Aprea, AROG, Daiichi Sankyo, and Pfizer; and received honoraria from Dava Oncology.
Correspondence: Aaron D. Goldberg, Leukemia Service, Division of Hematologic Malignancies, Department of Medicine, Memorial Sloan Kettering Cancer Center, 545 East 73rd St, New York, NY 10021; e-mail: goldbera@mskcc.org.

