

Key Points
DLBCL patients relapsing within 1 year of auto-HCT, and more importantly within 6 months of auto-HCT, have worse outcomes.
This study provides benchmarking for future trials of chimeric antigen receptor T cells and other agents evaluating PR-OS after auto-HCT.

Abstract
Outcomes for diffuse large B-cell lymphoma (DLBCL) patients relapsing after autologous hematopoietic cell transplantation (auto-HCT) have been historically poor. We studied outcomes of such patients using data from 4 transplantation centers. Eligibility criteria included adult patients (age ≥18 years) with DLBCL experiencing disease relapse after auto-HCT performed during 2006 to 2015. The time period was stratified into 2 eras (era 1, 2006-2010; era 2, 2011-2015). The primary end point was postrelapse overall survival (PR-OS). Secondary end points were factors prognostic of PR-OS. Of the 700 patients with DLBCL who underwent auto-HCT, 248 (35%) relapsed after auto-HCT. Median PR-OS of all relapsed DLBCL patients after auto-HCT (n = 228) was 9.8 months (95% confidence interval [CI], 7-15). Median PR-OS was significantly better for patients in complete (17.8 months; 95% CI, 7.9-41.6) vs partial remission at auto-HCT (7.1 months; 95% CI, 5.4-11; P = .01), those undergoing auto-HCT >1 year (12.8 months; 95% CI, 7.6-24.9) vs ≤1 year after DLBCL diagnosis (6.3 months; 95% CI, 4.5-9.2; P = .01), and those with late (56.4 months; 95% CI, 23.7-∞) vs early relapse (5.9 months; 95% CI, 4.5-8.8; P < .0001). On multivariate analysis, although late relapse (hazard ratio [HR], 0.21; 95% CI, 0.13-0.34; P < .0001) was associated with significantly lower mortality, the risk of mortality increased with age (HR, 1.25 per decade; 95% CI, 1.06-1.48; P = .009). This is the largest study to date to evaluate outcomes of DLBCL patients relapsing after auto-HCT. Our study provides benchmarking for future trials of chimeric antigen receptor T cells and other promising agents evaluating PR-OS after auto-HCT.
Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most common subtype of non-Hodgkin lymphoma (NHL), accounting for ∼30% of all NHL cases in the United States. In 2019, it is estimated that there will be 22 360 new cases diagnosed in the United States.1,2 Outcomes of DLBCL have improved since the introduction of rituximab, with ∼60% of patients now cured with rituximab-containing first-line therapy.3,4 However, despite this progress, 40% to 50% of DLBCL patients either fail to achieve remission with first-line therapy or relapse after achieving complete remission (CR). For relapsed/refractory DLBCL patients, treatment with salvage chemotherapy followed by autologous hematopoietic cell transplantation (auto-HCT) is potentially curative,5 although only ∼50% of patients who receive second-line salvage therapy demonstrate sufficient chemotherapy sensitivity to be candidates for auto-HCT. Furthermore, of those who do undergo auto-HCT, ∼50% will subsequently relapse. Contemporary registry data show that the relapse rate after auto-HCT has not improved since the results of the Parma trial,6-8 despite various strategies intended to improve outcomes.9-11
An expanding understanding of B-cell receptor biology in recent years has led to rapid growth in the number of novel agents available or undergoing evaluation for the treatment of relapsed/refractory DLBCL.12-20 However, studies focusing on the outcomes specifically of DLBCL patients relapsing after auto-HCT have been sparse. In the recently published SCHOLAR-1 study of relapsed/refractory DLBCL patients, median overall survival (OS) was 6.3 months. In that study, survival was measured starting from the time of initiation of salvage therapy.21 However, SCHOLAR-1 included patients who were primarily refractory to first- and second-line therapies and only a smaller proportion of patients who relapsed/progressed within 12 months after auto-HCT. There are 2 previously published studies evaluating post–auto-HCT relapse outcomes, in which a median OS post–auto-HCT relapse was reported to be in the range of 9 to 10 months.22,23 However, both of those studies were limited by small sample size and did not include patients treated in the contemporary time period.
Therefore, we sought to evaluate the outcomes of DLBCL patients relapsing after auto-HCT and determine the survival trends and factors prognostic of post–auto-HCT survival. We hypothesized that the outcomes of patients with DLBCL relapsing after auto-HCT may have improved in more recent years because of the availability of new/novel agents such as lenalidomide, ibrutinib, antibody/drug conjugates, and others that have activity in relapsed/refractory DLBCL.
Patients and methods
Study design
Adult patients (age ≥18 years) with relapsed/refractory (de novo) DLBCL who underwent auto-HCT between January 2006 and December 2015 at 4 academic tertiary care medical centers (Medical College of Wisconsin [Milwaukee, WI], The Ohio State University [Columbus, OH], Washington University School of Medicine [St. Louis, MO], and MD Anderson Cancer Center [Houston, TX]) were identified using clinical and transplantation databases. The Medical College of Wisconsin Scientific Review Committee and institutional review boards at all 4 sites approved this study. The study was performed in compliance with the Declaration of Helsinki.
To be eligible for the study, patients must have experienced disease relapse after auto-HCT (radiographic and/or histologically confirmed lymphoma relapse). Patients were selected after screening for eligibility criteria. After a retrospective chart review, patients were classified into 2 eras: era 1, 2006 to 2010 and era 2, 2011 to 2015. The year 2011 was chosen as the onset of the second era, because most of the data on novel agents for treatment of relapsed/refractory DLBCL came from around this time.12,13,16-18,20
Study end points and definitions
The primary end point was to determine post–auto-HCT relapse OS (PR-OS) in lymphoma patients experiencing relapse or progression after auto-HCT. The secondary end point was to identify factors prognostic of PR-OS.
PR-OS was measured from the time of documentation of DLBCL relapse or progression after auto-HCT to date of death or last follow-up. Time to relapse was defined as the time from auto-HCT to first documented evidence of DLBCL relapse or progression. Patients who relapsed at or within 1 year of auto-HCT were grouped into the early-relapse category, whereas those who relapsed beyond 1 year constituted the late-relapse group. Tumor assessment was performed according to individual center practices and not reviewed centrally.
Statistical analysis
Demographic and disease characteristics were summarized using descriptive statistics and compared between the cohorts using the Wilcoxon rank-sum test for continuous and ordinal measures and χ2 test for categorical outcomes. Patients were followed for survival from the time of post–auto-HCT relapse to death or last follow-up. Follow-up was administratively truncated at 6 years to better align the 2 cohorts. Survival curves were estimated using the Kaplan-Meier method and compared between groups via the log-rank test. Cox regression was used for the multivariable analysis of survival. The proportional hazards assumption was evaluated visually via residual plots and formally by introducing time-dependent effects, but no substantial deviations were found. The effect of the time-dependent treatment-start variables was visualized using several landmark times and analyzed in the Cox regression model as time-dependent covariates. Analyses were performed using SAS software (version 9.4; SAS Institute, Cary, NC).
Results
Patient characteristics
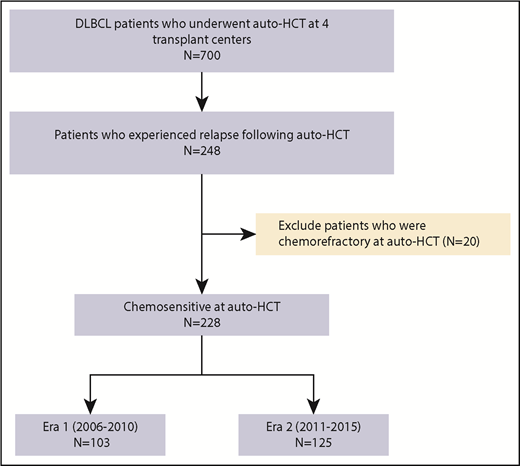
Of the 700 patients with de novo DLBCL who underwent auto-HCT at 1 of 4 participating academic centers in the United States, 248 (35%) relapsed post–auto-HCT between 2006 and 2015. After excluding patients who were chemotherapy refractory at auto-HCT (n = 20), 228 remained who were included in the analysis (era 1, n = 103; era 2, n = 125), as shown in Figure 1. Patient characteristics are listed in Table 1, with a breakdown between the 2 eras. Median age was 60 years, with male predominance (67%), and for all patients, the stem cell source was a peripheral blood hematopoietic progenitor cell graft. Median lines of therapy pre–auto-HCT was 2 (range, 1-4). Median time to relapse post auto-HCT was 6.1 months (range: 0.8–96.6 months). Median follow-up of survivors post–auto-HCT relapse (with the clock starting at relapse) was 39 months (range, 1-72 months). Of note, the main clinicobiologic variables that seemed to differ between DLBCL patients relapsing within 1 year after auto-HCT vs >1 year were time from diagnosis to auto-HCT and remission status at auto-HCT (supplemental Table 1).
Relapsed/refractory DLBCL patient characteristics
| P | ||||
|---|---|---|---|---|
| Entire group (n = 228) | 2006-2010 (n = 103) | 2011-2015 (n = 125) | ||
| Age at auto-HCT, y | .96 | |||
| Median | 60 | 59 | 60 | |
| Range | 25-77 | 32-77 | 25-77 | |
| Sex | .85 | |||
| Male | 152 (67) | 68 (66) | 84 (67) | |
| Female | 76 (33) | 35 (34) | 41 (33) | |
| ECOG PS at auto-HCT | .22 | |||
| 0 | 36 (17) | 17 (18) | 19 (16) | |
| 1 | 173 (80) | 76 (82) | 97 (79) | |
| 2 | 6 (3) | 0 | 6 (5) | |
| Missing | 13 | 10 | 3 | |
| DLBCL subtype | .76 | |||
| GCB | 38/66 (58) | 7/13 (54) | 31/53 (58) | |
| Non-GCB | 28/66 (42) | 6/13 (46) | 22/53 (42) | |
| DHL/THL | 9/91 (10) | 3/19 (16) | 6/72 (8) | .39 |
| Time from diagnosis to auto-HCT, y | .36 | |||
| ≤1* | 46 (20) | 18 (17) | 28 (22) | |
| >1 | 184 (80) | 85 (83) | 97 (78) | |
| Time from diagnosis to auto- HCT, mo | .28 | |||
| Median | 20.1 | 21.4 | 18.6 | |
| Range | 3.9-268 | 5.2-253 | 3.9-268 | |
| Lines of therapy before auto-HCT | .71 | |||
| Median | 2.0 | 2.0 | 2.0 | |
| Range | 1.0-4.0 | 1.0-4.0 | 1.0-4.0 | |
| Remission status at auto-HCT | .80 | |||
| CR | 115 (50) | 51 (50) | 64 (51) | |
| Partial remission | 113 (50) | 52 (50) | 61 (49) | |
| PB graft type | 228 (100) | 103 (100) | 125 (100) | — |
| Conditioning regimen | .29 | |||
| BEAM | 210 (92) | 97 (94) | 113 (90) | |
| Other | 18 (8) | 6 (6) | 12 (10) | |
| Timing of relapse after auto-HCT, y | .53 | |||
| ≤1 | 151 (66) | 66 (64) | 85 (68.0) | |
| >1 | 77 (34) | 37 (36) | 40 (32.0) | |
| Time from auto-HCT to relapse, mo | .22 | |||
| Median | 6.2 | 6.4 | 6.1 | |
| Range | 0.8-96.6 | 0.9-96.6 | 0.8-60.2 | |
| Salvage therapy post auto-HCT relapse | ||||
| Lines of therapy | ||||
| Median | 1 | 1 | 1 | |
| Range | 0-9 | 0-6 | 0-9 | |
| Lenalidomide | 41/228 (18) | 15/103 (15) | 26/125 (21) | .22 |
| Ibrutinib | 15/228 (7) | 4/103 (4) | 11/125 (9) | .14 |
| Checkpoint inhibitors | 8/220 (4) | 1/103 (1) | 7/125 (6) | .08 |
| Allogeneic HCT | 48/228 (21) | 26/103 (25) | 22/125 (18) | .16 |
| Clinical trials† | 38/228 (17) | 15/103 (15) | 23/125 (19) | .44 |
| FU post–auto-HCT relapse, mo | ||||
| Median | 39 | 63 | 35 | |
| Range | 1-72 | 5-72 | 1-72 | |
| P | ||||
|---|---|---|---|---|
| Entire group (n = 228) | 2006-2010 (n = 103) | 2011-2015 (n = 125) | ||
| Age at auto-HCT, y | .96 | |||
| Median | 60 | 59 | 60 | |
| Range | 25-77 | 32-77 | 25-77 | |
| Sex | .85 | |||
| Male | 152 (67) | 68 (66) | 84 (67) | |
| Female | 76 (33) | 35 (34) | 41 (33) | |
| ECOG PS at auto-HCT | .22 | |||
| 0 | 36 (17) | 17 (18) | 19 (16) | |
| 1 | 173 (80) | 76 (82) | 97 (79) | |
| 2 | 6 (3) | 0 | 6 (5) | |
| Missing | 13 | 10 | 3 | |
| DLBCL subtype | .76 | |||
| GCB | 38/66 (58) | 7/13 (54) | 31/53 (58) | |
| Non-GCB | 28/66 (42) | 6/13 (46) | 22/53 (42) | |
| DHL/THL | 9/91 (10) | 3/19 (16) | 6/72 (8) | .39 |
| Time from diagnosis to auto-HCT, y | .36 | |||
| ≤1* | 46 (20) | 18 (17) | 28 (22) | |
| >1 | 184 (80) | 85 (83) | 97 (78) | |
| Time from diagnosis to auto- HCT, mo | .28 | |||
| Median | 20.1 | 21.4 | 18.6 | |
| Range | 3.9-268 | 5.2-253 | 3.9-268 | |
| Lines of therapy before auto-HCT | .71 | |||
| Median | 2.0 | 2.0 | 2.0 | |
| Range | 1.0-4.0 | 1.0-4.0 | 1.0-4.0 | |
| Remission status at auto-HCT | .80 | |||
| CR | 115 (50) | 51 (50) | 64 (51) | |
| Partial remission | 113 (50) | 52 (50) | 61 (49) | |
| PB graft type | 228 (100) | 103 (100) | 125 (100) | — |
| Conditioning regimen | .29 | |||
| BEAM | 210 (92) | 97 (94) | 113 (90) | |
| Other | 18 (8) | 6 (6) | 12 (10) | |
| Timing of relapse after auto-HCT, y | .53 | |||
| ≤1 | 151 (66) | 66 (64) | 85 (68.0) | |
| >1 | 77 (34) | 37 (36) | 40 (32.0) | |
| Time from auto-HCT to relapse, mo | .22 | |||
| Median | 6.2 | 6.4 | 6.1 | |
| Range | 0.8-96.6 | 0.9-96.6 | 0.8-60.2 | |
| Salvage therapy post auto-HCT relapse | ||||
| Lines of therapy | ||||
| Median | 1 | 1 | 1 | |
| Range | 0-9 | 0-6 | 0-9 | |
| Lenalidomide | 41/228 (18) | 15/103 (15) | 26/125 (21) | .22 |
| Ibrutinib | 15/228 (7) | 4/103 (4) | 11/125 (9) | .14 |
| Checkpoint inhibitors | 8/220 (4) | 1/103 (1) | 7/125 (6) | .08 |
| Allogeneic HCT | 48/228 (21) | 26/103 (25) | 22/125 (18) | .16 |
| Clinical trials† | 38/228 (17) | 15/103 (15) | 23/125 (19) | .44 |
| FU post–auto-HCT relapse, mo | ||||
| Median | 39 | 63 | 35 | |
| Range | 1-72 | 5-72 | 1-72 | |
Data are n (%) unless otherwise indicated.
BEAM, carmustine, etoposide, cytarabine, and melphalan; ECOG, Eastern Cooperative Oncology Group; DHL, double-hit lymphoma; GCB, germinal center B-cell subtype; PS, performance status; THL, triple-hit lymphoma.
Patients with very early relapse after first-line therapy, those who achieved less than CR with first-line therapy, or those who were refractory to first-line therapy.
Information regarding specific agents was available in 28 patients; of these, 21 patients received small-molecule–targeted therapies, 4 patients received drug-antibody conjugates, and 3 patients received other therapies (azacytadine, n = 2; AZD9150, n = 1).
Treatment at relapse
Salvage therapy at relapse after auto-HCT was based on physician discretion at the individual academic centers (Table 1). Median lines of therapy for DLBCL patients post–auto-HCT relapse was 1 (range, 0-9). The most common salvage therapies administered were allogeneic HCT (21%), lenalidomide (18%), and clinical trial participation (17%). Of note, although the predominant salvage therapy post–auto-HCT relapse in era 1 was allogeneic HCT (25%), lenalidomide (21%) was the most commonly used salvage modality after auto-HCT relapse in era 2 (Table 1).
PR-OS
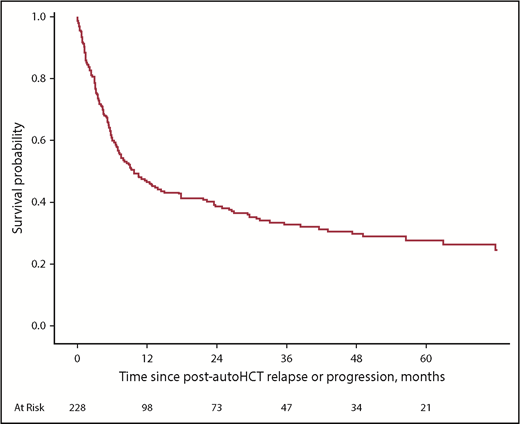
Median PR-OS of all relapsed DLBCL patients after auto-HCT (n = 228) was 9.8 months (95% confidence interval [CI], 7-15), with 1-year PR-OS of 46% (95% CI, 40-53), 3-year PR-OS of 33% (95% CI, 26-39), and 5-year PR-OS of 28% (95% CI, 21-34; Figure 2). When PR-OS was assessed based on remission status at auto-HCT, median PR-OS for patients in CR was 17.8 months (95% CI, 7.9-41.6), which was significantly longer than that for patients who were in partial remission going into auto-HCT (7.1 months; 95% CI, 5.4-11; P = .01; Figure 3).

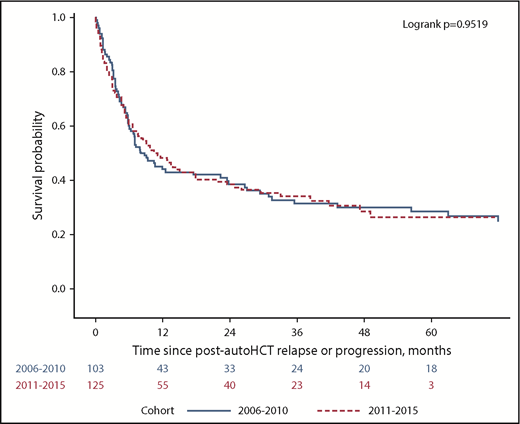
Median PR-OS was significantly better for patients undergoing auto-HCT >1 year after DLBCL diagnosis (12.8 months; 95% CI, 7.6-24.9) vs within 1 year of diagnosis (6.3 months; 95% CI, 4.5-9.2; P = .01; supplemental Figure 1) and for patients with late relapse (56.4 months; 95% CI, 23.7-∞) vs early relapse (5.9 months; 95% CI, 4.5-8.8; P < .0001; Figure 4A). On detailed analysis of the timing of relapse after auto-HCT, median PR-OS for patients relapsing within 3, 3 to 6, and 6 to 12 months after auto-HCT was 4.1 (95% CI, 3.2-5.2), 7.3 (95% CI, 3.8-11.5), and 17.8 months (95% CI, 7.2-43.2), respectively (Figure 4B). For patients who relapsed >12 months after auto-HCT, median PR-OS was 56.4 months (95% CI, 23.7 to not reached). Of note, there was no significant difference in median PR-OS based on era of auto-HCT (era 1 vs era 2, 8 months; 95% CI, 5.9-22.3 vs 11 months; 95% CI, 6.6-17.9, respectively; P = .95; Figure 5).
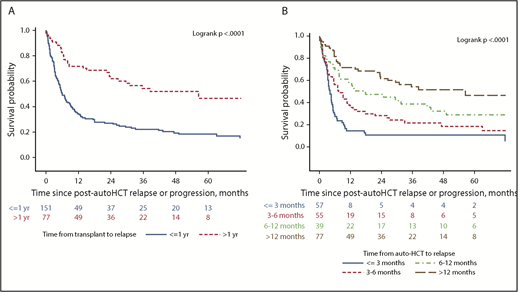
PR-OS based on timing of relapse after auto-HCT. (A) Within 1 year vs >1 year after auto-HCT. (B) Detailed breakdown of PR-OS within 1 year vs >1 year after auto-HCT.
PR-OS based on timing of relapse after auto-HCT. (A) Within 1 year vs >1 year after auto-HCT. (B) Detailed breakdown of PR-OS within 1 year vs >1 year after auto-HCT.
Factors prognostic of PR-OS
Variables included in the multivariate analysis were era of auto-HCT, age at auto-HCT, Eastern Cooperative Oncology Group performance status at auto-HCT, disease status at auto-HCT, time from auto-HCT to relapse, allogeneic HCT, and clinical trial participation. On multivariate analysis (Table 2), although late relapse (HR, 0.21; 95% CI, 0.13-0.34; P < .0001) was associated with significantly lower mortality, the risk of mortality increased with age (HR, 1.25 per decade; 95% CI, 1.06-1.48; P = .009). There was some evidence that patients who were in CR at auto-HCT had improved survival (HR, 0.75; 95% CI, 0.54-1.03; P = .07). Of note, there was no significant effect of postrelapse clinical trial participation (supplemental Figure 2A) or allogeneic HCT on PR-OS (supplemental Figure 2B).
Factors prognostic of PR-OS on multivariate analysis
| HR | 95% CI | P | |
|---|---|---|---|
| Age at auto-HCT, decades | 1.25 | 1.06-1.48 | .009 |
| Timing of relapse post–auto-HCT, mo | |||
| ≤3 | 1 | ||
| 3-6 | 0.56 | 0.36-0.84 | .006 |
| 6-12 | 0.37 | 0.23-0.61 | <.0001 |
| >12 | 0.21 | 0.13-0.34 | <.0001 |
| Disease status at auto-HCT | |||
| Partial response | 1 | .07 | |
| CR | 0.75 | 0.54-1.03 |
| HR | 95% CI | P | |
|---|---|---|---|
| Age at auto-HCT, decades | 1.25 | 1.06-1.48 | .009 |
| Timing of relapse post–auto-HCT, mo | |||
| ≤3 | 1 | ||
| 3-6 | 0.56 | 0.36-0.84 | .006 |
| 6-12 | 0.37 | 0.23-0.61 | <.0001 |
| >12 | 0.21 | 0.13-0.34 | <.0001 |
| Disease status at auto-HCT | |||
| Partial response | 1 | .07 | |
| CR | 0.75 | 0.54-1.03 |
Variables included in multivariate analysis: era of auto-HCT, age at auto-HCT, Eastern Cooperative Oncology Group performance status at auto-HCT, disease status at auto-HCT, time from auto-HCT to relapse, allogeneic HCT, and clinical trial participation.
HR, hazard ratio.
Subset analysis
Among the 228 patients relapsing after auto-HCT, 151 (66%) relapsed at or within 1 year. There was no difference in median PR-OS when comparing the early-relapse group between era 1 (5.3 months; 95% CI, 3.5-7.2) and era 2 (7.5 months; 95% CI, 4.7-11; P = .65; supplemental Figure 3A). Seventy-seven patients (34%) relapsed beyond 1 year after auto-HCT. There was no difference in PR-OS when comparing the late-relapse group between era 1 (56.4 months; 95% CI, 23.5-∞) and era 2 (not reached; 95% CI, 15-∞; P = .95; supplemental Figure 3B). Although median PR-OS was longer for patients who were in CR at auto-HCT in era 2 (21.7 months; 95% CI, 9.2-47.2) relative to era 1 (10.6 months; 95% CI, 5.7-71.8), the difference was not statistically significant (P = .78; supplemental Figure 4A). There was no significant difference in median PR-OS for patients who were in partial remission at auto-HCT in era 1 (7.2 months; 95% CI, 4.3-17.4) vs era 2 (6.8 months; 95% CI, 5.1-12.8; P = .96; supplemental Figure 4B). Although median PR-OS was longer in patients without double-hit lymphoma/triple-hit lymphoma (n = 91; 17.8 months; 95% CI, 9.1-41.6) vs with double-hit lymphoma/triple-hit lymphoma (n = 9; 5.5 months; 95% CI, 1.2-∞), the difference was not statistically significant (P = .47), probably because of small sample size (supplemental Figure 5).
Discussion
Prospective studies evaluating the outcomes of DLBCL patients after auto-HCT relapse have not been performed. Here, we performed a multicenter retrospective cohort study of DLBCL patients relapsing after auto-HCT in the contemporaneous era and made several important observations. First, there has been no significant improvement in PR-OS in the most recent era. Second, factors prognostic of significantly poor PR-OS include advanced age at auto-HCT and relapse within 1 year of auto-HCT. Lastly, we could not discern the impact of clinical trial participation or allogeneic HCT on PR-OS. In our study, the rate of post–auto-HCT relapse was 35%, which is lower than the 50% noted in the previous studies.5-7 This difference is likely due to the fact that all patients in the current study received rituximab-based frontline treatment and were chemotherapy sensitive at auto-HCT.
With a better molecular understanding of DLBCL biology, a number of novel agents have been introduced in recent years, which have activity in relapsed/refractory DLBCL. These treatments include immunomodulatory agents,12 BTK inhibitors,13 proteasome inhibitors,14 PI3K/AKT/mTOR pathway inhibitors,15,16 antibody-drug conjugates,17 immune checkpoint inhibitors,18,19 BCL2 inhibitors,20 and others. However, despite the higher use of novel and investigational agents in the most recent era (55% vs 35%), median PR-OS remained poor (9.8 months; 95% CI, 7-14.4). This observation is in line with previously published studies22,23 showing continued poor outcomes in DLBCL patients who progress after auto-HCT, even in more recent years.
DLBCL patients relapsing within 1 year of auto-HCT had worse prognosis, with a median PR-OS of 5.9 months, which has not significantly improved in the most recent era. Our results are in line with previously published studies including the post–auto-HCT relapse group (defined by relapse within 1 year of auto-HCT) of the SCHOLAR-121 study (6.2 months).21-23 On detailed analysis, we noted that among patients relapsing within 1 year of auto-HCT, poor outcomes were predominantly driven by patients relapsing within 6 months of auto-HCT. Alhough median PR-OS was slightly better in patients relapsing within 6 months and 6 to 12 months after auto-HCT relative to the previous study, where median PR-OS for patients relapsing within 6 months and 6 to 12 months were 5.7 and 11.3 months, respectively23 ; outcomes continue to remain dismal in this patient population. For patients relapsing >12 months after auto-HCT, median PR-OS was significantly longer (56.4 months). For this group of patients, a detailed discussion may be required regarding consideration of alternatives to chimeric antigen receptor (CAR) T-cell therapy, such as allogeneic HCT or nontransplantation/noncellular therapies. Median PR-OS was better in patients who were in CR (relative to those in partial response) at the time of auto-HCT, which is in line with previous studies.22,23 However, this did not translate into a significant factor prognostic of PR-OS in the multivariable analysis. The current study provides a breakdown of data in a more granular way than in previous studies in the post–auto-HCT relapse setting and should provide helpful benchmarking for the post–auto-HCT relapse patients who make up a significant proportion of the many CAR T-cell and related trials of relapsed/refractory DLBCL currently taking place.
Allogeneic HCT provides a potentially curative option (via graft-versus-lymphoma effect) for DLBCL patients who progress after auto-HCT, with nearly 40% of carefully selected patients achieving long-term remission.24 However, only ∼20% of DLBCL patients who fail auto-HCT ultimately proceed to allogeneic HCT,25 and more importantly, the procedure has a high associated risk of therapy-related complications; the associated rate of death unrelated to disease relapse is ∼20% to 25% at 1 year.24,25 In our study, we did not note any significant impact of allogeneic HCT on PR-OS; however, the results need to be interpreted with caution, given the small number of patients. Additionally, there could have been significant selection bias for patients undergoing allogeneic HCT, which could have altered the results.
Therapeutic T-cell engineering (eg, CAR T-cell therapy) has recently garnered widespread interest because of the success of CD19 CAR therapy. CARs are synthetic receptors for antigens that redirect the specificity and reprogram the function of the T cells into which they are genetically introduced. Studies have shown very good response rates with CAR T-cell therapy in the refractory DLBCL patient population, with durable responses in a significant subset of those achieving CR.26,27 However, only 2126 and 54 patients27 had undergone prior auto-HCT in these studies, and outcomes of this particular patient population relative to those of other relapsed/refractory groups are unclear. Nevertheless, CAR T-cell therapy is a promising option in patients relapsing post–auto-HCT. The current study provides benchmarking for future studies (post–CAR T-cell era) investigating PR-OS after auto-HCT.
Given the retrospective nature of this study, our study has important limitations. Because of the small proportion of patients receiving ibrutinib and checkpoint inhibitors in the post–auto-HCT relapse setting, further analysis of the impact of these agents on PR-OS could not be performed. We did not have information on the revised international prognostic index (secondary international prognostic index) or c-MYC rearrangement at relapse, thereby precluding their inclusion in the multivariable model. Response to the therapies administered in the post–auto-HCT relapse setting was assessed by the treating physician, and the information pertaining to assessment of response (positron emission tomography vs computed tomography scan) to these therapies was not available. Although type of imaging modality (positron emission tomography vs computed tomography scan) used could have had an impact on response to post–auto-HCT relapse treatments, we believe that this would not ultimately have had an impact on PR-OS. Lastly, outcomes of patients enrolled in clinical trials may be difficult to interpret because of multiple factors that can potentially influence enrollment, including Eastern Cooperative Oncology Group performance status, organ function, and nature of the trial (phase 1 vs 2), despite controlling for patient-, disease-, and transplantation-related variables by using landmark analysis and multivariable modeling.
Notwithstanding these limitations, this is the largest study to date to evaluate the outcomes of DLBCL patients relapsing after auto-HCT. DLBCL patients who relapse within 1 year of auto-HCT, and more importantly within 6 months of auto-HCT, experience worse outcomes and represent an urgent unmet need. CAR T-cell therapy may benefit this patient population; however, additional data are needed to evaluate the impact of CAR T-cell therapy for patients relapsing post–auto-HCT. Our study provides benchmarking for future trials of CAR T cells and other promising agents evaluating PR-OS after auto-HCT.
The full-text version of this article contains a data supplement.
Authorship
Contribution: N.E. and T.S.F. were responsible for conception and design; N.E., A.S., and T.S.F. performed data analysis; N.E. wrote the first draft of the manuscript; and all authors performed collection and assembly of data, interpreted the data, provided critical and insightful comments, and provided final approval of the manuscript.
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Correspondence: Narendranath Epperla, Division of Hematology, Department of Medicine, The Ohio State University, 320 W 10th Ave, Columbus, OH 43210; e-mail: narendranath.epperla@osumc.edu.

