Background
The prevalence of sickle cell disease (SCD) in the Republic of Uganda is higher than in the United States, but there are no accurate countrywide data and no newborn screening program has been established. The Early Infant Diagnosis (EID) program is well established to analyze dried blood spots (DBSs) collected from HIV-exposed infants (ie, those born to HIV-positive mothers). HIV-positive infants are identified and placed into specialty care.
At the request of the Uganda Ministry of Health, a partnership was developed between Cincinnati Children’s Hospital Medical Center, Makerere University, and the Uganda Central Public Health Laboratories (CHPL) to build local laboratory capacity for testing DBSs for sickle cell trait (SCT) and SCD.
The Uganda Sickle Surveillance Study (US3) was designed to identify SCT or SCD in DBSs collected throughout the national EID program. After US3, screening commenced in high-burden districts with local capacity built to provide clinical care for affected infants.
Objectives
To build local capacity for laboratory skills with the following specific objectives:
Establish a national sickle cell laboratory with appropriate equipment and reagents,
Train local technologists to test all DBSs received by the EID program, and
Analyze the data to determine the countrywide burden and create a geospatial map of SCT and SCD.
To build local capacity to improve clinical management of SCD with the following specific objectives:
Perform educational training workshops in high-burden districts,
Teach local health care providers about the rationale and benefits of testing at-risk children for SCD, and
Initiate public awareness through health fairs and radio announcements to boost screening efforts.
Forming the partnership
Uganda Ministry of Health
Commissioned up-to-date data across the country regarding the sickle cell burden,
Prioritized high-burden districts to provide limited resources for sickle cell interventions and improvements through primary care, and
Offered to leverage health policy agendas and mobilize funding for sustainable sickle cell services.
Uganda CPHL identified local laboratory technologists for training
Procured all reagents with in-country vendors and
Launched the US3 study and the follow-on sickle cell testing campaign.
Cincinnati Children’s Hospital Medical Center
Purchased all required laboratory equipment and reagents to launch the US3 project;
Provided technical expertise in sickle cell testing methodologies and training, including weekly Skype calls with quality assessments; and
Conducted remote monitoring and analysis of results to curate data in real time.
Makerere University College of Health Sciences
Provided an academic home for the sickle screening efforts including local institutional review board approvals,
Facilitated announcement and discussion of the main results at the end of the US3 study, and
Performed educational training in high-burden districts to increase screening and to establish local sickle cell clinics at the district hospitals.
Initial US3 screening results
US3
In all, 97 631 samples were tested from 2014 to 2015 (Table 1).
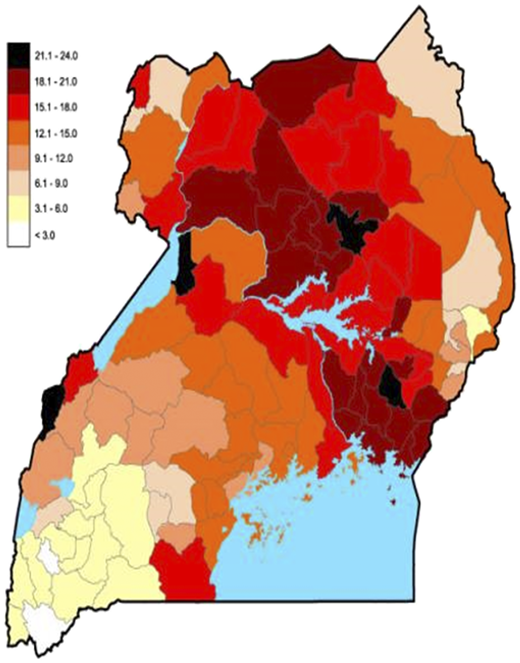
The overall prevalence of SCT was 13.3% and the prevalence of SCD was distribution was noted across Uganda with the highest burden in central regions.
Screening and training efforts
Initiation in selected districts with the highest prevalence of SCT and SCD.
Wave 1 (October 2014) included Gulu and Lira districts with high populations.
Wave 2 (April-May 2015) included Dokolo, Jinja, Kampala, Kitgum, Oyam, and Tororo.
Wave 3 (July-August 2016) included Alebtong, Agago, Amolatar, Apac, Bundibugyo, Lamwo, Luwero, Mityana, Mubende, and Pader.
Education and community outreach
Sickle cell education and training about diagnostic testing and the new CPHL screening program was made available for health care providers.
Affected infants and children were referred to local district hospitals for specialized care, using teaching guidelines provided by national health care experts.
Program fundraising efforts included an annual Buganda Kingdom Fun Run and Outreach screening events.
World Sickle Cell Day celebration was held on June 19.
Post-US3 screening results
Targeted screening of high-burden districts
112 352 samples were tested from 2015 to 2018 (Table 1).
The prevalence of SCT (15.5%) and SCD (1.3%) was higher than in the original US3 study.
Uganda National Sickle Cell Laboratory
After the local laboratory reached its maximum capacity, the new CPHL was expanded to include a large sickle cell laboratory.
This laboratory offers free sickle cell testing to babies, toddlers, and adults.
Upcoming research objectives
Obtain follow-up data on babies identified with SCD;
Explore the observed comorbidity between SCD and HIV;
Characterize hemoglobin variants identified during sickle cell surveillance efforts;
Characterize genetic modifiers of SCD such as alpha-thalassemia trait or G6PD deficiency, using DNA-based technology; and
Investigate isolated districts with high or low prevalence of SCT to determine the influence of environmental, social, and genetic factors.





Prevalence of sickle cell trait in 112 districts in Uganda. Reproduced from Ndeezi G et al, Lancet Glob Health. 2016;4(3):e195-e200, with permission.
Prevalence of sickle cell trait in 112 districts in Uganda. Reproduced from Ndeezi G et al, Lancet Glob Health. 2016;4(3):e195-e200, with permission.

Authorship
Conflict-of-interest disclosures: R.E.W. received research funding from Addmedica, Bristol-Myers Squibb, and Biomedomics; served as a consultant for Nova Laboratories; was a member of the board of directors and served on an advisory committee for Novartis; and served on an advisory committee for Global Blood Therapeutics and Agios. The remaining authors have no competing financial interests to declare.
Correspondence: Charles Kiyaga, Central Public Health Laboratories, Ministry of Health, Kampala, Uganda; e-mail: ckiyaga@gmail.com.