

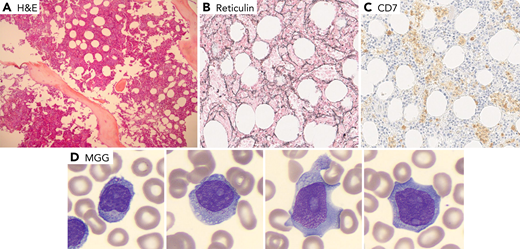
A 68-year-old patient was admitted for increased splenomegaly after 6 months of treatment with ruxolitinib for primary myelofibrosis (PMF). No JAK2 V617F/exon12- MPL- CAL-R or other mutations were detected in next-generation sequencing analysis (77 genes panel). Bone marrow biopsy showed increased cellularity (panel A, original magnification ×100) with grade 2 myelofibrosis based on reticulin stain (panel B, original magnification ×200). There was no improvement after addition of hydroxyurea. The blood cell count on admission showed mild neutropenia and thrombocytopenia, a discrete hyperlymphocytosis (4-5 × 109/L) with presence of abnormal lymphocytes on the blood film, some with cytoplasmic granules, others with a blastic appearance with nucleoli (panel D, original magnification ×1000). The flow cytometry analysis showed 85% natural killer (NK) cells, CD7+/sCD3−/CD2+/CD5−/CD4−/CD8−/CD56+/CD16+ low/CD57−. The diagnosis of aggressive NK cell leukemia was made. Histological review of the initial bone marrow biopsy showed interstitial and sinusoidal infiltration by NK cells (panel C, CD7 stain, original magnification ×200). Karyotyping of peripheral blood cells showed a hypodiploid complex karyotype. The disease progressed rapidly despite 2 lines of treatment.
This case reminds us that myelofibrosis is not only seen in myeloproliferative neoplasms. Careful histological analysis should be performed in triple-negative PMF to not miss clues for other diagnoses.
A 68-year-old patient was admitted for increased splenomegaly after 6 months of treatment with ruxolitinib for primary myelofibrosis (PMF). No JAK2 V617F/exon12- MPL- CAL-R or other mutations were detected in next-generation sequencing analysis (77 genes panel). Bone marrow biopsy showed increased cellularity (panel A, original magnification ×100) with grade 2 myelofibrosis based on reticulin stain (panel B, original magnification ×200). There was no improvement after addition of hydroxyurea. The blood cell count on admission showed mild neutropenia and thrombocytopenia, a discrete hyperlymphocytosis (4-5 × 109/L) with presence of abnormal lymphocytes on the blood film, some with cytoplasmic granules, others with a blastic appearance with nucleoli (panel D, original magnification ×1000). The flow cytometry analysis showed 85% natural killer (NK) cells, CD7+/sCD3−/CD2+/CD5−/CD4−/CD8−/CD56+/CD16+ low/CD57−. The diagnosis of aggressive NK cell leukemia was made. Histological review of the initial bone marrow biopsy showed interstitial and sinusoidal infiltration by NK cells (panel C, CD7 stain, original magnification ×200). Karyotyping of peripheral blood cells showed a hypodiploid complex karyotype. The disease progressed rapidly despite 2 lines of treatment.
This case reminds us that myelofibrosis is not only seen in myeloproliferative neoplasms. Careful histological analysis should be performed in triple-negative PMF to not miss clues for other diagnoses.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal