

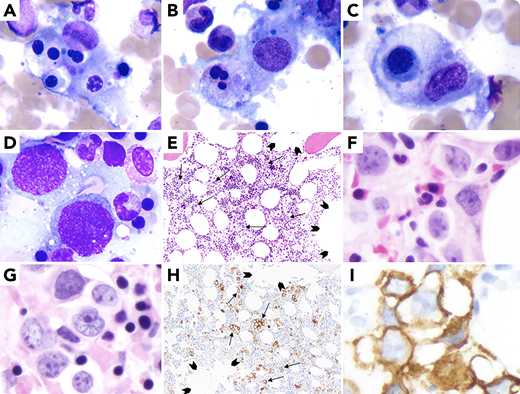
A 67-year-old woman presented with fatigue, fever (38.6°C), bicytopenia (platelets 9 × 103/µL; hemoglobin 9.6 g/dL), elevated ferritin (4313 ng/mL)/triglycerides (481 mg/dL)/interleukin-2 receptor (CD25: 87 950.0 pg/mL), cytomegalovirus viremia, and positive nasal swab for methicillin-resistant Staphylococcus aureus. A computed tomography scan showed hepatosplenomegaly without lymphadenopathy. Bone marrow aspirate smears showed hemophagocytic histiocytes (panels A-C: May-Grunwald-Giemsa, 100× objective, ×1000 magnification), large cells (panel D: May-Grunwald-Giemsa, 100× objective, ×1000 magnification), and negative flow cytometry. Trephine biopsy showed large cell infiltrate (panel E: hematoxylin and eosin (H&E), ×10X objective, 100× magnification; and panels F, G: H&E, 40× objective, ×400 magnification) with CD20 expression showing interstitial (not intravascular/intrasinusoidal) infiltration by lymphoma cells (arrows) and uninvolved sinusoids (arrowheads) (panel H: CD20, 10× objective, ×100 magnification showing interstitial distribution of large B cells; and panel I: CD20, 40× objective, ×400 magnification)/Bcl-2/Bcl-6/MUM1/MYC (not shown) and negative for CD10/CD5/cyclin-D1/CD30/ALK-1/TdT/CD34. Primary bone marrow diffuse large B-cell lymphoma (nongerminal center B cell) with hemophagocytic lymphohistiocytosis (HLH) was diagnosed (splenomegaly/fever/elevated ferritin/hypertriglyceridemia/elevated CD25/hemophagocytosis on aspirate met 6 of 8 criteria). Cytogenetics showed complex karyotype. After chemotherapy and antimicrobial coverage for methicillin-resistant S aureus and cytomegalovirus infections, the patient is doing well.
The case illustrates the importance of having a very high index of suspicion for malignancy in older patients with HLH even if there are other possible nonmalignant (eg, infections) causes of HLH for appropriate therapy.
A 67-year-old woman presented with fatigue, fever (38.6°C), bicytopenia (platelets 9 × 103/µL; hemoglobin 9.6 g/dL), elevated ferritin (4313 ng/mL)/triglycerides (481 mg/dL)/interleukin-2 receptor (CD25: 87 950.0 pg/mL), cytomegalovirus viremia, and positive nasal swab for methicillin-resistant Staphylococcus aureus. A computed tomography scan showed hepatosplenomegaly without lymphadenopathy. Bone marrow aspirate smears showed hemophagocytic histiocytes (panels A-C: May-Grunwald-Giemsa, 100× objective, ×1000 magnification), large cells (panel D: May-Grunwald-Giemsa, 100× objective, ×1000 magnification), and negative flow cytometry. Trephine biopsy showed large cell infiltrate (panel E: hematoxylin and eosin (H&E), ×10X objective, 100× magnification; and panels F, G: H&E, 40× objective, ×400 magnification) with CD20 expression showing interstitial (not intravascular/intrasinusoidal) infiltration by lymphoma cells (arrows) and uninvolved sinusoids (arrowheads) (panel H: CD20, 10× objective, ×100 magnification showing interstitial distribution of large B cells; and panel I: CD20, 40× objective, ×400 magnification)/Bcl-2/Bcl-6/MUM1/MYC (not shown) and negative for CD10/CD5/cyclin-D1/CD30/ALK-1/TdT/CD34. Primary bone marrow diffuse large B-cell lymphoma (nongerminal center B cell) with hemophagocytic lymphohistiocytosis (HLH) was diagnosed (splenomegaly/fever/elevated ferritin/hypertriglyceridemia/elevated CD25/hemophagocytosis on aspirate met 6 of 8 criteria). Cytogenetics showed complex karyotype. After chemotherapy and antimicrobial coverage for methicillin-resistant S aureus and cytomegalovirus infections, the patient is doing well.
The case illustrates the importance of having a very high index of suspicion for malignancy in older patients with HLH even if there are other possible nonmalignant (eg, infections) causes of HLH for appropriate therapy.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal