

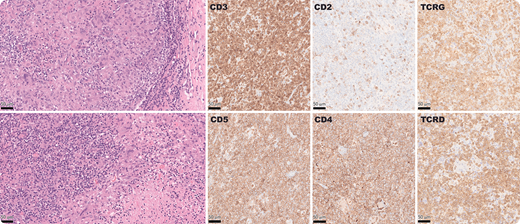
A 78-year-old man presented with multiregional lymphadenopathy and 20-pound weight loss. Inguinal lymph node biopsy showed effaced architecture by a polymorphous population of atypical lymphoid cells of varying size, associated with necrotizing granulomas with multinucleated giant cells and admixed plasma cells. Atypical T cells were positive for CD3, CD5, CD4, CD43, MUM1, TCRD, and TCRG with partial loss of CD2, and CD7, while negative for ALK1, BCL2, BCL6, β-F1, CD8, CD10, CD25, CD56, CD161(NK1.1), CXCL13, ICOS, granzyme B, PD1, TdT, and TIA1 by immunohistochemistry. EBER-ISH and HHV8 were negative. No microorganisms were detected. Polymerase chain reaction showed clonal TRG, IGH, and IGK gene rearrangement within a polyclonal background. TSO500-NGS showed TP53 p.V143M, KDM6A p.S531fs*21, CDKN2A exon1-3 deletion, and CDKN2B exon1-2 deletion.
This novel peripheral T-cell lymphoma exhibited a γδ phenotype. It is unusual for γδ T cells to express CD4, because γδ T cells mostly develop from CD4−/CD8− double-negative thymocytes. However, the atypical T cells in this case retained some of the normal features of T-cell development. CD5−/NK1.1+ γδ T cells are transformed to CD5+/NK1.1− during host defense against infection. In addition, γδ T cells showing high levels of interferon-γ (IFN-γ) production are normally negative for BCL2, CD25, and CD161. IFN-γ production can result in granuloma formation as was prominent in this case. Images were taken with 40× objective; ×400 total magnification. The 50-μm scale is shown as a black bar.
A 78-year-old man presented with multiregional lymphadenopathy and 20-pound weight loss. Inguinal lymph node biopsy showed effaced architecture by a polymorphous population of atypical lymphoid cells of varying size, associated with necrotizing granulomas with multinucleated giant cells and admixed plasma cells. Atypical T cells were positive for CD3, CD5, CD4, CD43, MUM1, TCRD, and TCRG with partial loss of CD2, and CD7, while negative for ALK1, BCL2, BCL6, β-F1, CD8, CD10, CD25, CD56, CD161(NK1.1), CXCL13, ICOS, granzyme B, PD1, TdT, and TIA1 by immunohistochemistry. EBER-ISH and HHV8 were negative. No microorganisms were detected. Polymerase chain reaction showed clonal TRG, IGH, and IGK gene rearrangement within a polyclonal background. TSO500-NGS showed TP53 p.V143M, KDM6A p.S531fs*21, CDKN2A exon1-3 deletion, and CDKN2B exon1-2 deletion.
This novel peripheral T-cell lymphoma exhibited a γδ phenotype. It is unusual for γδ T cells to express CD4, because γδ T cells mostly develop from CD4−/CD8− double-negative thymocytes. However, the atypical T cells in this case retained some of the normal features of T-cell development. CD5−/NK1.1+ γδ T cells are transformed to CD5+/NK1.1− during host defense against infection. In addition, γδ T cells showing high levels of interferon-γ (IFN-γ) production are normally negative for BCL2, CD25, and CD161. IFN-γ production can result in granuloma formation as was prominent in this case. Images were taken with 40× objective; ×400 total magnification. The 50-μm scale is shown as a black bar.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal