

TO THE EDITOR:
Bruton's tyrosine kinase (BTK) inhibitors and the BCL-2 antagonist venetoclax have significantly improved the outcome of patients with chronic lymphocytic leukemia (CLL).1 Nonetheless, high-risk patients with 17p deletion (del17p) and/or TP53 mutations have an increased risk for treatment failure with BTK inhibitors in relapsed or refractory (R/R) CLL2 and with venetoclax in first-line3 and relapsed CLL therapy4 when compared with patients with lower-risk features. For example, the median progression-free survival (PFS) of heavily pretreated R/R patients with CLL receiving ibrutinib in the PCYC-1102 study was 52 months, but it was only 26 months for those with del17p and/or TP53 mutations.2 The duration of remission is longer when BTK inhibitors are used in earlier lines of therapy, especially in patients with CLL who are treatment-naïve. Importantly, other CLL high-risk features (unmutated IGHV, del11q) no longer predict for inferior outcome when ibrutinib is used as first-line therapy for CLL, and consequently these high-risk patients have survival outcomes that are equivalent to those of patients with low-risk CLL.5 Whether this also applies to patients with CLL who have TP53 aberrations is not well established, because these patients were excluded from pivotal CLL first-line trials.5,6 Recently, long-term outcome from a cohort of 34 treatment-naïve patients with CLL and TP53 alterations reported a 6-year PFS of 61% and overall survival (OS) of 79%.7 Here, we report the long-term outcome of 27 treatment-naïve patients with CLL and del17p and/or TP53 mutations who are receiving ibrutinib alone or in combination with rituximab on an investigator-initiated phase 2 trial. This trial was registered at www.clinicaltrials.gov as #NCT02007044. The trial was approved by The University of Texas MD Anderson Cancer Center Institutional Review Board, and informed consent was obtained in accordance with institutional guidelines and the Declaration of Helsinki.
A cohort of 27 treatment-naïve patients with CLL and del17p and/or TP53 mutation was part of a phase 2 randomized study that compared single-agent ibrutinib with ibrutinib plus rituximab for patients with high-risk CLL. This trial was conducted at MD Anderson Cancer Center and enrolled a total of 208 patients, 181 of whom had R/R CLL (51 patients with del17p or TP53 mutation) and 27 treatment-naïve patients with del17p or TP53 mutation. The outcome of the trial, which reported a similar outcome in both treatment arms (PFS of 86% with ibrutinib and 86.9% with ibrutinib plus rituximab) after a median follow-up of 36 months, was reported earlier by Burger et al8 in Blood. Among the untreated patients with TP53 alterations, 15 received ibrutinib as a single agent and 12 received the combination of ibrutinib and rituximab. PFS was defined as the time from start of treatment to progression, death, or last follow-up. Survival curves and median time to response were calculated by using the Kaplan and Meier method, and univariable comparisons were made with the log-rank test. All tests were 2-sided, and results were considered significant if P ≤ .05. Baseline demographic and clinical characteristics are summarized in Table 1.
Baseline demographic and clinical characteristics of treatment-naïve patients
| Characteristic | No. (N = 27) | % | Median | Range |
|---|---|---|---|---|
| Age ≥70 years | 3 | 11 | 62 | 48-79 |
| Sex | ||||
| Male | 18 | 67 | ||
| Female | 9 | 33 | ||
| ECOG performance status* | ||||
| 0 | 1 | 4 | ||
| 1 | 26 | 96 | ||
| Rai stage† | ||||
| 0, I, or II | 18 | 67 | ||
| III or IV | 9 | 33 | ||
| IGHV mutational status | ||||
| Mutated | 3 | 11 | ||
| Unmutated | 21 | 78 | ||
| Data missing | 4 | 11 | ||
| ZAP-70 (IHC) | ||||
| Negative | 9 | 33 | ||
| Positive | 17 | 63 | ||
| Data missing | 1 | 4 | ||
| β2-microglobulin >3.5 mg/L | 16 | 59 | 4.0 | 2.0-13.1 |
| White blood cell count × 109/μL | 96.6 | 8.8-321.4 | ||
| Hemoglobin, g/dL | 12.6 | 8.1-16.3 | ||
| Platelets × 109/μL | 162 | 77-292 |
| Characteristic | No. (N = 27) | % | Median | Range |
|---|---|---|---|---|
| Age ≥70 years | 3 | 11 | 62 | 48-79 |
| Sex | ||||
| Male | 18 | 67 | ||
| Female | 9 | 33 | ||
| ECOG performance status* | ||||
| 0 | 1 | 4 | ||
| 1 | 26 | 96 | ||
| Rai stage† | ||||
| 0, I, or II | 18 | 67 | ||
| III or IV | 9 | 33 | ||
| IGHV mutational status | ||||
| Mutated | 3 | 11 | ||
| Unmutated | 21 | 78 | ||
| Data missing | 4 | 11 | ||
| ZAP-70 (IHC) | ||||
| Negative | 9 | 33 | ||
| Positive | 17 | 63 | ||
| Data missing | 1 | 4 | ||
| β2-microglobulin >3.5 mg/L | 16 | 59 | 4.0 | 2.0-13.1 |
| White blood cell count × 109/μL | 96.6 | 8.8-321.4 | ||
| Hemoglobin, g/dL | 12.6 | 8.1-16.3 | ||
| Platelets × 109/μL | 162 | 77-292 |
IHC, immunohistochemistry.
Eastern Cooperative Oncology Group (ECOG) performance status ranges from 0 to 5, with 0 indicating no symptoms and higher numbers indicating increasing disability.
Rai stage 0 indicates low-risk, stage I or II intermediate-risk, and stage III or IV high-risk disease.
The median age of the patients with untreated CLL and TP53 alterations (del17p and/or TP53 mutations) was 62 years (range, 48-79 years), and 21 patients (78%) had unmutated IGHV genes (Table 1). After a median follow-up of 70 months (range, 5-85 months), 9 patients (33%) remained on study. Median PFS and OS were not reached; the estimated 6-year PFS was 60% and the estimated OS was 79% (Figure 1 A-B). This is markedly better than the 5-year PFS of 15.3% in patients with CLL and del17p after treatment with fludarabine, cyclophosphamide, and rituximab.9 Subset analyses in the Alliance A041202 trial that compared outcome of treatment-naïve patients with CLL and del17p and/or TP53 mutations who were receiving bendamustine plus rituximab (n = 14), ibrutinib monotherapy (n = 9), or ibrutinib plus rituximab (n = 11) also demonstrated strikingly better outcomes for patients on the ibrutinib arms.10 Patients with CLL and del17p (n = 17) or TP53 deletion and/or mutation (n = 25) who were receiving first-line venetoclax plus obinutuzumab have an estimated 36-month PFS of 48.5% or 60.4%, respectively.3 PFS and OS for patients receiving ibrutinib alone vs the combination of ibrutinib plus rituximab are provided in supplemental Figure 1. Although we noted longer PFS and OS in treatment-naïve patients receiving the combination of ibrutinib plus rituximab (supplemental Figure 1A-B, available on the Blood Web site), the PFS differences were not statistically significant, and the deaths of patients receiving ibrutinib monotherapy were not considered disease- or treatment-related (supplemental Table 1). PFS and OS of patients with R/R CLL and del17p and/or TP53 mutations were similar for patients in both treatment arms (supplemental Figure 1C-D); the disease progression and death events in this cohort of patients are detailed in supplemental Table 2. PFS and OS for the entire cohort of 208 patients with CLL who received ibrutinib alone or ibrutinib plus rituximab are provided in supplemental Figure 2C-D. There were no significant differences in PFS and OS when comparing treatment-naïve patients with CLL and del17p and/or TP53 mutations (n = 27) with the remaining cohort of patients who had R/R CLL (n = 181; supplemental Figure 3A-B) or when comparing treatment-naïve patients with R/R CLL (n = 51) with patients with CLL and del17p and/or TP53 mutations, even though there was a trend for shorter PFS and OS in the R/R cohort (Figure 1C-D).
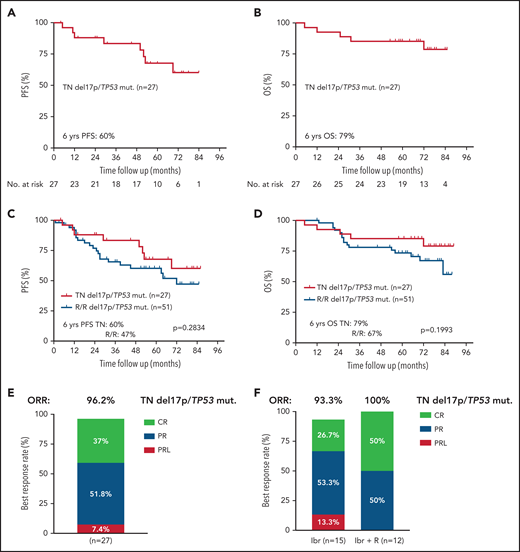
Survival and responses in treatment-naïve (TN) and patients with R/R CLL and del17p and/or TP53 mutations (mut) receiving ibrutinib (Ibr) alone or in combination with rituximab (R). (A) PFS and (B) OS of TN patients with CLL and del17p and/or TP53 mutations (n = 27). (C) PFS and OS (D) of TN CLL patients vs patients with R/R CLL and del17p and/or TP53 mutations. (E) Best responses in the TN patients with del17p and/or TP53 mutations. (F) Best responses in further subset analyses based on treatment (ibrutinib monotherapy/Ibr vs ibrutinib plus rituximab/Ibr + R).
Survival and responses in treatment-naïve (TN) and patients with R/R CLL and del17p and/or TP53 mutations (mut) receiving ibrutinib (Ibr) alone or in combination with rituximab (R). (A) PFS and (B) OS of TN patients with CLL and del17p and/or TP53 mutations (n = 27). (C) PFS and OS (D) of TN CLL patients vs patients with R/R CLL and del17p and/or TP53 mutations. (E) Best responses in the TN patients with del17p and/or TP53 mutations. (F) Best responses in further subset analyses based on treatment (ibrutinib monotherapy/Ibr vs ibrutinib plus rituximab/Ibr + R).
The most common reason for treatment discontinuation was disease progression, which occurred in 6 patients (22%): 2 had histologically confirmed Richter’s transformation and 4 had progressive CLL, with a median time to progression of 39 months (range, 10-53 months). The second most common reason for treatment discontinuation was a change to an alternative therapy per physician’s choice in 5 patients (19%) (venetoclax plus ibrutinib in 4 patients, acalabrutinib in 1 patient). Two patients discontinued treatment because of recurrent atrial fibrillation, and 2 other patients developed a secondary malignancy (prostate cancer or glioblastoma multiforme). Other reasons for therapy discontinuation were new onset of idiopathic thrombocytopenic purpura (1 patient) or persistent lymphocytosis (1 patient). Death occurred in 5 patients (18%), 2 of whom died as a result of disease progression (Richter’s transformation or CLL progression with respiratory failure). Because the vast majority of the patients who came off study proceeded immediately to alternative treatments, we cannot comment about outcome of treatment discontinuation. Only 1 patient who discontinued ibrutinib plus rituximab after 14 months of therapy as a result of atrial fibrillation (with achievement of a CR with undetectable minimal residual disease) has remained in remission since 2016, with last follow-up in 2020.
Objective responses were noted in all but 1 patient (ORR, 96.2%), with CRs in 10 patients (37%), partial remissions (PRs) in 14 patients (51.8%), and PR with lymphocytosis (PRL) in 2 patients (7.4%). Among the 15 patients who received ibrutinib alone, 4 (26.7%) achieved a CR, 8 (53.3%) achieved a PR, and 2 (13.3%) achieved a PRL as best response, accounting for an ORR of 93.3%. Among the 12 patients treated with ibrutinib plus rituximab, 6 (50%) achieved a CR (3 with undetectable minimal residual disease), which was maintained while the patients were on study, and 6 (50%) achieved a PR, accounting for an ORR of 100% (Figure 1E-F).
Response assessment at different time points showed similar response rates among the evaluable patients at 12 months (CR rate, 25%) and 24 months (CR rate, 29%) of continued therapy. Median levels of bone marrow CLL cells declined from 76% at baseline (95% confidence interval [CI], 73%-85%) to 26% (95% CI, 3.5%-50%; P < .001) after 12 months, and 14% (95% CI, 0.8%-22.4%; P < .001) after 24 months of therapy (supplemental Figure 4A-B).
The duration of remission was not different in patients achieving CR (n = 10) or PR (n = 16), suggesting that deep remissions are not a prerequisite for durable remissions. However, the sample size in these subgroups is small, and therefore, larger cohorts of patients are needed to validate these results (supplemental Figure 5). Venetoclax-based therapy, which generally induces deeper remissions, does not seem to induce more durable remissions (3-year PFS, 48.5% with venetoclax plus obinutuzumab in treatment-naïve patients with CLL and del17p and/or TP53 mutations),3 although cross-trial comparisons are problematic, especially given that venetoclax was administered as a fixed-duration regimen. Future research, as in the CLL17 trial, which compares ibrutinib monotherapy with venetoclax plus obinutuzumab or venetoclax plus ibrutinib, will determine whether combination therapy results in an improvement in survival. In summary, our data demonstrate that first-line therapy with ibrutinib results in long-term remissions in patients with high-risk CLL patients who have del17p and/or TP53 mutations, corroborating recent data7 that BTK inhibitor monotherapy is providing durable remissions in this high-risk population of patients with CLL.
Acknowledgments
The authors thank the patients who participated in this trial and their families, the study investigators, and the study coordinator (Thomas Mathew) at the MD Anderson Cancer Center.
This work was supported by Pharmacyclics (an AbbVie company), philanthropic contributions to The University of Texas MD Anderson Cancer Center Moon Shots Program, the CLL Global Research Foundation, and, in part, by a grant from the National Institutes of Health, National Cancer Institute (CA016672).
Authorship
Contribution: J.A.B. designed and supervised the trial, analyzed the data, and wrote the paper with M.S.; W.G.W., A.F., N.J., P.T., H.K., and M.K. contributed to the trial design, clinical patient management, sample collection, and clinical data analysis and reviewed and approved the manuscript; and M.S. and E.K. performed data collection and statistical analyses.
Conflict-of-interest disclosure: J.A.B., N.J., and P.T. received research funding from Pharmacyclics and served as consultants for Janssen Pharmaceuticals. N.J. and P.T. have served as consultants for AbbVie, and N.J. has served as a consultant for Pharmacyclics. P.T. received funding from AbbVie. The remaining authors declare no competing financial interests.
Correspondence: Jan A. Burger, Department of Leukemia, Unit 428, The University of Texas MD Anderson Cancer Center, PO Box 301402, Houston, TX 77230-1402; e-mail: jaburger@mdanderson.org.
The online version of this article contains a data supplement.
For access to publication-related data, please contact Jan A. Burger via e-mail at jaburger@mdanderson.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal