

A 58-year-old man presented with a complaint of left flank pain. He had no significant past medical history. Laboratory study showed normal complete blood count and chemistry. Physical examination revealed splenomegaly, but no hepatomegaly or lymphadenopathy. CT scan showed a low-density mass in the posterior spleen, which raised suspicion for partially thrombosed hemangioma on magnetic resonance imaging. The patient underwent robotic splenectomy. Gross examination showed a well circumscribed mass measuring 8.5 cm in dimension (panel A). The histology showed sheets of tumor cells with monotonous appearance. They were small to intermediate in size with round nuclear contours, open chromatin and small but distinct nucleoli. Coagulative necrosis and frequent mitosis were seen (panels B and C, hematoxylin and eosin stain, original magnification ×100 and ×400, respectively). The cells were positive for CD20, BCL-6, MUM-1, and P53 protein but negative for CD3, CD5, CD10, BCL-1, BCL-2, and MYC protein by immunohistochemistry. Ki-67 (proliferation index) highlighted >95% of tumor cells. Fluorescence in situ hybridization analysis was negative for MYC/BCL-2/BCL-6 gene rearrangements but positive for 11q aberration, which was further confirmed by chromosomal microarray (panel D, chromosomal 11q23.3-q24.3 gain and 11q25 loss).
Burkitt-like lymphoma with 11q aberration is recognized as a distinct entity by the recent World Health Organization classification. It is germinal center derived and genetically unrelated to typical Burkitt lymphoma. This aggressive lymphoma usually presents in lymph node/soft tissue. Primary splenic manifestation is extremely uncommon.
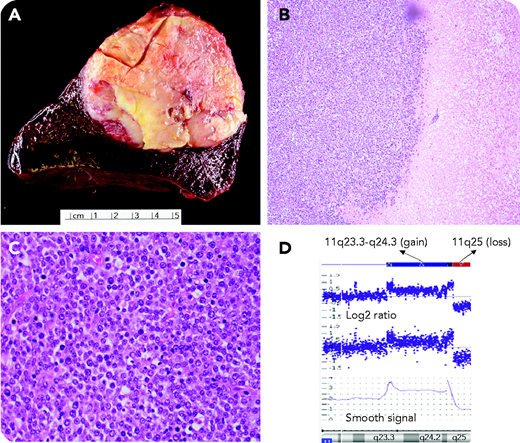
A 58-year-old man presented with a complaint of left flank pain. He had no significant past medical history. Laboratory study showed normal complete blood count and chemistry. Physical examination revealed splenomegaly, but no hepatomegaly or lymphadenopathy. CT scan showed a low-density mass in the posterior spleen, which raised suspicion for partially thrombosed hemangioma on magnetic resonance imaging. The patient underwent robotic splenectomy. Gross examination showed a well circumscribed mass measuring 8.5 cm in dimension (panel A). The histology showed sheets of tumor cells with monotonous appearance. They were small to intermediate in size with round nuclear contours, open chromatin and small but distinct nucleoli. Coagulative necrosis and frequent mitosis were seen (panels B and C, hematoxylin and eosin stain, original magnification ×100 and ×400, respectively). The cells were positive for CD20, BCL-6, MUM-1, and P53 protein but negative for CD3, CD5, CD10, BCL-1, BCL-2, and MYC protein by immunohistochemistry. Ki-67 (proliferation index) highlighted >95% of tumor cells. Fluorescence in situ hybridization analysis was negative for MYC/BCL-2/BCL-6 gene rearrangements but positive for 11q aberration, which was further confirmed by chromosomal microarray (panel D, chromosomal 11q23.3-q24.3 gain and 11q25 loss).
Burkitt-like lymphoma with 11q aberration is recognized as a distinct entity by the recent World Health Organization classification. It is germinal center derived and genetically unrelated to typical Burkitt lymphoma. This aggressive lymphoma usually presents in lymph node/soft tissue. Primary splenic manifestation is extremely uncommon.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal