

TO THE EDITOR:
Patients with multiple myeloma (MM) are at an increased risk for infection because of their immunocompromised state, old age, and comorbidities.1 Coronavirus disease 2019 (COVID-19) causes moderate to severe acute respiratory dysfunction in 77% of patients with MM, and ∽8% end up in critical condition.2 More than 80% of patients with MM who are infected by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) require hospitalization,3 whereas ∽33% of hospitalized MM patients with COVID-19 may die because of the infection.4 This is mainly due to the limited therapeutic options for COVID-19.5
Vaccination against SARS-CoV-2 could be an important preventive strategy against COVID-19 for patients with MM, but its efficacy in MMis largely unknown.6 The BNT162b2 messenger RNA (mRNA) vaccine is the first anti–SARS-CoV-2 vaccine approved by the US Food and Drug Administration and the European Medicines Agency as a result of its high efficacy in apparently healthy adults.7 Recently, it was reported that the first BNT162b2 dose provided some protection against COVID-19 among nursing facility residents.8,9 However, there is no information in the literature about its efficacy in patients with MM or with other malignant diseases. Herein, we report the development of neutralizing antibodies (NAbs) against SARS-CoV-2 in patients with MM after the first dose of the BNT162b2 vaccine.
Major inclusion criteria for the participation of patients with MM in this study included age >18 years; presence or smoldering myeloma or active MM, irrespective of the treatment given or the line of therapy; and eligibility for vaccination, according to International Myeloma Society recommendations.8 Volunteers of similar age and sex, who served as controls, were included in this analysis. Major exclusion criteria for myeloma patients and controls included the presence of autoimmune disorders or active malignant disease, HIV or active hepatitis B and C infection, or end-stage renal disease. Herein, we report a sub-analysis of a prospective study (NCT04743388) evaluating the kinetics of anti–SARS-CoV-2 antibodies following COVID-19 vaccination in healthy subjects and patients with hematological malignancies or solid tumors.
After vein puncture, serum of patients and controls was collected on day 1 (D1; before the first BNT162b2 dose) and on day 22 (D22; before the second dose of the vaccine). Serum was separated within 4 hours of blood collection and stored at −80°C until the day of measurement. NAbs against SARS-CoV-2 were measured using methodology approved by the US Food and Drug Administration (enzyme-linked immunosorbent assay; cPass SARS-CoV-2 Neutralizing Antibody Detection Kit; GenScript, Piscataway, NJ)10 at the above time points. Samples from the same patient or control were measured in the same enzyme-linked immunosorbent assay plate. The study was approved by the institutional Ethical Committees in accordance with the Declaration of Helsinki and the International Conference on Harmonization for Good Clinical Practice. All patients and controls provided informed consent before entering into the study.
The current study population included 48 patients with MM (29 males/19 females; median age, 83 years; range, 59-92 years) and 104 controls (57 males/47 females; median age, 83 years; range, 65-95 years), who were vaccinated during the same period at the same vaccination center (Alexandra Hospital, Athens, Greece). The advanced age of the participants was the result of the Greek vaccination program that prioritizes octogenarians and health care workers for COVID-19 immunization.
The characteristics of the patients with myeloma are depicted in Table 1. In summary, at the time of vaccination, 35 (72.9%) patients were receiving antimyeloma therapy, 4 were in remission after prior therapy and did not receive any therapy at the time of vaccination, and 9 had smoldering myeloma.
Characteristics of patients with MM
| Total patients (males/females), n | 48 (29/19) |
| Age, median (range), y | 83 (59-92) |
| Smoldering myeloma/active myeloma | 9 (18.7)/39 (81.2) |
| Receiving treatment for active myeloma, yes/no, n | 35/4 |
| Line of therapy, if on treatment (n = 35) | |
| First | 15 (42.9) |
| Second | 10 (28.6) |
| Third | 4 (11.4) |
| Greater than third | 6 (17.1) |
| Type of therapy | |
| PI+IMiD combos | 9 (25.7) |
| VRD | 6 |
| IRD | 2 |
| PomVD | 1 |
| IMiD-based regimens | 14 (40.0) |
| Rd | 10 |
| R maintenance | 2 |
| RCd | 1 |
| PomCd | 1 |
| PI-based regimens | 2 (5.7) |
| VD | 1 |
| ICD | 1 |
| Anti-CD38 mAb-based therapies | 8 (22.8) |
| Daratumumab monotherapy | 4 |
| Daratumumab-Rd | 2 |
| Daratumumab-PomDex | 1 |
| Isatuximab-Rd | 1 |
| Belantamab mafodotin monotherapy | 2 (5.7) |
| Total patients (males/females), n | 48 (29/19) |
| Age, median (range), y | 83 (59-92) |
| Smoldering myeloma/active myeloma | 9 (18.7)/39 (81.2) |
| Receiving treatment for active myeloma, yes/no, n | 35/4 |
| Line of therapy, if on treatment (n = 35) | |
| First | 15 (42.9) |
| Second | 10 (28.6) |
| Third | 4 (11.4) |
| Greater than third | 6 (17.1) |
| Type of therapy | |
| PI+IMiD combos | 9 (25.7) |
| VRD | 6 |
| IRD | 2 |
| PomVD | 1 |
| IMiD-based regimens | 14 (40.0) |
| Rd | 10 |
| R maintenance | 2 |
| RCd | 1 |
| PomCd | 1 |
| PI-based regimens | 2 (5.7) |
| VD | 1 |
| ICD | 1 |
| Anti-CD38 mAb-based therapies | 8 (22.8) |
| Daratumumab monotherapy | 4 |
| Daratumumab-Rd | 2 |
| Daratumumab-PomDex | 1 |
| Isatuximab-Rd | 1 |
| Belantamab mafodotin monotherapy | 2 (5.7) |
Unless otherwise noted, data are n (%).
ICD, ixazomib, cyclophosphamide and dexamethasone; IMiD, immunomodulatory drug; IRD, ixazomib, lenalidomide, and dexamethasone; mAb, monoclonal antibody; PI, proteasome inhibitor; PomCd, pomalidomide, cyclophosphamide, and dexamethasone; PomVD, pomalidomide, bortezomib, and dexamethasone; PomDex, pomalidomide and dexamethasone; R, lenalidomide; RCd, lenalidomide, cyclophosphamide, and dexamethasone; Rd, lenalidomide and dexamethasone; VD, bortezomib and dexamethasone; VRD, bortezomib, lenalidomide and dexamethasone.
On D1, no patient or control had NAb titers ≥30% (the cutoff defining positivity); similarly, there was no difference with regard to NAb titers between patients with MM and controls on D1. After the first dose of the vaccine, on D22, patients with MM had lower NAb titers compared with controls: median NAb-inhibition titers was 20.6% (range, 0-96.7%) for patients with MM vs 32.5% (range, 5.2-97.3%) for controls (P < .01; Figure 1). More specifically, only 12 (25.0%) patients with MM vs 57 (54.8%) controls developed NAb titers ≥30% on D22. Four (8.3%) patients with MM and 21 (20.2%) controls developed NAb titers ≥50% (which corresponds to clinically relevant viral inhibition).11 All 4 patients with MM were in remission without receiving any antimyeloma therapy: 3 patients after frontline therapy with bortezomib, lenalidomide, and dexamethasone (2 patients had achieved a very good partial response and 1 had achieved a partial response on the day of the administration of the first dose of the vaccine) and 1 patient after second-line treatment with lenalidomide and dexamethasone for 14 months (the patient had achieved a very good partial response on D1 of the vaccination). These 4 patients also had normal levels of the uninvolved immunoglobulins after treatment. No other correlation was observed between the antimyeloma treatment given and the development of NAb titers on D22.
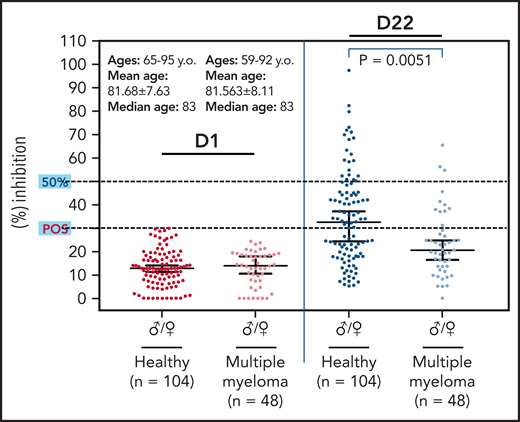
Kinetics of NAbs in elderly patients with myeloma and age-matched controls after vaccination with the first dose of the BNT162b2 mRNA vaccine. On D22, patients with myeloma had lower production of NAb inhibition titers compared with controls of similar age and sex. Only 4 patients with myeloma had NAb titers ≥50%. POS, positivity threshold.
Kinetics of NAbs in elderly patients with myeloma and age-matched controls after vaccination with the first dose of the BNT162b2 mRNA vaccine. On D22, patients with myeloma had lower production of NAb inhibition titers compared with controls of similar age and sex. Only 4 patients with myeloma had NAb titers ≥50%. POS, positivity threshold.
Interestingly, only 1 (11.1%) of 9 patients with smoldering myeloma had NAb titers ≥30% (positivity cutoff) vs 11 (28.2%) of 39 patients with active MM. This patient had normal levels of the uninvolved immunoglobulins, whereas the other 8 patients had immunoparesis in ≥1 uninvolved immunoglobulin. This observation is of great interest, because hypoglobulinemia has been associated with an inferior antibody response among patients with chronic lymphocytic leukemia and COVID-19.12
Our data indicate that the first dose of BNT162b2 leads to production of lower levels of NAbs against SARS-CoV-2 among patients with MM compared with non-MM controls of similar age and sex and without malignant disease. This may be due to the effect of myeloma cells, which suppress normal B-cell expansion and immunoglobulin production. Furthermore, some antimyeloma therapies have a B-cell–depleting activity that, in turn, may impair immune response to vaccines, whereas the myeloma microenvironment and antimyeloma treatments may impair T-cell function.13 Patients with MM often exhibit suboptimal seroconversion rates after a single-dose vaccine against bacteria and viruses; therefore, booster doses are needed to assure adequate protection, such as with the seasonal flu vaccine.13 We should also take into consideration that the production of NAb titers against SARS-CoV-2 at a level ≥50% on D21 after the first BNT162b2 dose has been low, even among healthy individuals aged 65 to 85 years.11 However, higher antibody titers after a single dose of mRNA-based vaccine against SARS-CoV-2 have been detected in individuals who have recovered from COVID-19.9 Because our results indicate that elderly myeloma patients have a blunted antibody response after the first vaccine dose, they also suggest that the administration of a second timely vaccine dose is essential to develop an adequate antibody-based immune response in this elderly subpopulation with a malignant hematological disease that deregulates the immune homeostasis. Antimyeloma therapy seems to negatively affect NAb production (after a single dose), although larger patient numbers are needed to evaluate the effects of specific antimyeloma regimens on the immune responses of anti–SARS-CoV-2 vaccination. Furthermore, this low antibody response of elderly patients with myeloma after the first BNT162b2 dose may not be seen in younger patients. Our ongoing study will also answer this question.
Acknowledgments
The authors thank Ioanna Rentziou, Ioanna Charitaki, Tina Bagratuni, Christine Ivy Liacos, and Nikoletta-Aikaterini Kokkali for administrative, technical, or material support, and Sentiljana Gumeni and Filia Apostolakou for acquisition, analysis, or interpretation of data. They also thank all of the study participants for donating their time and samples.
This work was supported, in part, by SYN-ENOSIS, AEGEAS, and IEMBITHEK.
Authorship
Contribution: E.T. designed and performed research, analyzed data, and wrote the manuscript; I.P.T. and M.A.D. contributed vital new reagents or analytical tools, performed research, analyzed data, and reviewed all drafts of the manuscript and approved the final version; and I.P., A.D.S., I.N.-S., E.-D.P., D.F., M.G., and E.K. performed research, analyzed data, reviewed all drafts of the manuscript and approved the final version.
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Correspondence: Evangelos Terpos, Department of Clinical Therapeutics, National and Kapodistrian University of Athens, School of Medicine, Alexandra General Hospital, 80 Vas. Sofias Ave, 11528 Athens, Greece; e-mail: eterpos@med.uoa.gr.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal