

Key Points
The addition of brentuximab vedotin was tolerable and prevented relapses, and EFS compares favorably with conventional chemotherapy.
The study confirmed that minimal disseminated disease detection in peripheral blood was prognostic, with a significant impact on EFS.

Abstract
Approximately 30% of pediatric patients with anaplastic large cell lymphoma (ALCL) relapse. Although brentuximab vedotin has demonstrated excellent activity in ALCL, it has not been used for newly diagnosed patients. Children’s Oncology Group (COG) trial ANHL12P1 determined the toxicity and efficacy of brentuximab vedotin with chemotherapy in children with newly diagnosed nonlocalized anaplastic large cell lymphoma kinase (ALK)+/CD30+ ALCL. From 2013 to 2017, 68 children with ALK+ ALCL were enrolled and received brentuximab vedotin. All patients received 5-day prophase, followed by 6 cycles of chemotherapy. Brentuximab vedotin was given on day 1 of each of the 6 cycles. Of the 67 patients eligible for toxicity evaluation, 66 completed all 6 cycles of chemotherapy, resulting in 399 evaluable cycles. There were no toxic deaths, no case of progressive multifocal leukoencephalopathy syndrome, and no case of grade 3 or 4 neuropathy. The 2-year event-free survival (EFS) was 79.1% (95% confidence interval [CI], 67.2-87.1). The 2-year overall survival (OS) was 97.0% (95% CI, 88.1-99.2). Fourteen patients relapsed. Eleven of 14 (79%) relapses occurred within 10 months of diagnosis; only 1 patient (1.5%) relapsed during therapy. Quantitative reverse transcription polymerase chain reaction for NPM-ALK at baseline (minimal disseminated disease) demonstrated prognostic value for EFS (P = .0004). Overall, the addition of brentuximab vedotin to standard chemotherapy does not add significant toxicity or alter the desired interval between cycles. The addition of brentuximab vedotin prevented relapses during therapy, and the OS and EFS estimates compare favorably with results obtained using conventional chemotherapy. This trial was registered at www.clinicaltrials.gov as #NCT01979536.
Introduction
Anaplastic large cell lymphoma (ALCL) is a distinct form of non-Hodgkin lymphoma that accounts for 10% to 15% of all childhood lymphomas.1-3 ALCL is a mature T-cell lymphoma that is characterized by pleomorphic tumor cells and strong expression of CD30.4 The World Health Organization now classifies ALCL as separate entities based on the expression of the anaplastic large cell lymphoma kinase (ALK) oncogene: ALK+ ALCL and ALK− ALCL.5 In children, >95% of cases of ALCL are ALK+. Pediatric ALCL is characterized by advanced disease at presentation, with a high incidence of extranodal involvement.6,7
Numerous treatment strategies have been investigated in clinical trials utilizing a number of chemotherapeutic agents, as well as a wide range of therapy duration (Table 1).3,8-16 No approach has been able to improve on the approximate failure rate of 30% that exists, regardless of the treatment strategy. In addition, progression while receiving chemotherapy portends a very poor prognosis in children with ALCL, with only 25% to 41% of patients who progress on therapy expected to survive, even with aggressive salvage therapy, including bone marrow transplantation.17-19 Therefore, early interventions that prevent on-therapy disease progression should have the greatest impact on overall survival (OS).
Clinical trial results for pediatric ALCL
| Treatment strategy | No. of patients | Age, median (range), y | Treatment duration (months) | EFS (%) | Study |
|---|---|---|---|---|---|
| B-cell strategy with COPADM + maintenance | 82 | 10 (1.4-17) | 8 | 66 | Brugieres et al, 19989 |
| B-cell strategy with BFM-90 | 89 | 10.5 (0.8-17.3) | 5 | 76 | Seidemann et al, 20013 |
| B-cell strategy with COPADM | 72 | 11.8 (1.1-16.4) | 7-8 | 59 | Williams et al, 200216 |
| T-cell leukemia therapy | 34 | 11.6 (4.2-14.9) | 24 | 65 | Rosolen et al, 200515 |
| APO | 86 | NR | 12 | 72 | Laver et al, 200511 |
| Intensive T-cell strategy | 86 | NR | 12 | 68 | Lowe et al, 200913 |
| ALCL99 (B-cell strategy) | 352 | 11 (0.3-19.5) | 5 | 74 | Brugieres et al, 200920 |
| B-cell strategy BFM-95 | 32 | 10 (0.6-17.6) | 5 | 68 | Pillon et al, 201214 |
| APO with randomization of VBL | 125 | 11.9 (0.7-20) | 12 | 76 | Alexander et al, 20148 |
| Treatment strategy | No. of patients | Age, median (range), y | Treatment duration (months) | EFS (%) | Study |
|---|---|---|---|---|---|
| B-cell strategy with COPADM + maintenance | 82 | 10 (1.4-17) | 8 | 66 | Brugieres et al, 19989 |
| B-cell strategy with BFM-90 | 89 | 10.5 (0.8-17.3) | 5 | 76 | Seidemann et al, 20013 |
| B-cell strategy with COPADM | 72 | 11.8 (1.1-16.4) | 7-8 | 59 | Williams et al, 200216 |
| T-cell leukemia therapy | 34 | 11.6 (4.2-14.9) | 24 | 65 | Rosolen et al, 200515 |
| APO | 86 | NR | 12 | 72 | Laver et al, 200511 |
| Intensive T-cell strategy | 86 | NR | 12 | 68 | Lowe et al, 200913 |
| ALCL99 (B-cell strategy) | 352 | 11 (0.3-19.5) | 5 | 74 | Brugieres et al, 200920 |
| B-cell strategy BFM-95 | 32 | 10 (0.6-17.6) | 5 | 68 | Pillon et al, 201214 |
| APO with randomization of VBL | 125 | 11.9 (0.7-20) | 12 | 76 | Alexander et al, 20148 |
APO, doxorubicin, prednisone, vincristine, methotrexate, 6‐mercaptopurine; BFM, Berlin-Frankfort-Munster; COPADM, cyclophosphomide, vincristine, prednisone, doxorubicin, methotrexate; EFS, event-free survival; NR, not recorded; VBL, vinblastine.
CD30 is a transmembrane glycoprotein receptor that is expressed on all systemic ALCL in children, making it an ideal target for therapy. Brentuximab vedotin is a CD30-directed antibody conjugated to monomethyl auristatin E (MMAE). Brentuximab vedotin binds to CD30, becomes internalized, and releases MMAE, which causes apoptosis as an antitubulin agent. Tubulin inhibitors are active against ALCL, as evidenced by responses using vinblastine.19,20 Brentuximab vedotin has demonstrated activity as a single agent (1.8 mg/kg every 3 weeks) in pediatric patients (>12 years) with relapsed ALCL, with objective response rates of 53% to 86% in phase 1 and 2 settings.21,22 The most common toxicities in adults and children were nausea, fatigue, pyrexia, and hematological toxicities. Peripheral neuropathy is a common dose-limiting event in adults who receive brentuximab vedotin, whereas it is seemingly more transient with limited severity in children.22,23
The primary aim of arm BV (addition of brentuximab vedotin to standard chemotherapy) of Children’s Oncology Group (COG) trial ANHL12P1 (ANHL12P1) was to determine the tolerability of treatment and to estimate the event-free survival (EFS) and OS.
Patients and methods
Study design
ANHL12P1 was a randomized phase 2 study with the primary aim to determine the toxicity and efficacy in arm BV and arm CZ (addition of crizotinib to standard chemotherapy) in children with newly diagnosed nonlocalized ALK+/CD30+ ALCL. The results of arm BV are reported here; the results of arm CZ will be the subject of a future report. ANHL12P1 was approved by the National Cancer Institute Central Institutional Review Board and the institutional review boards of participating institutions. Informed consent for study participants was obtained from participants (or parents or guardians) prior to starting protocol therapy, in accordance with the US Department of Health and Human Services guidelines.
Patients
Eligible patients had histologically proven ALK+ ALCL and were younger than 22 years of age at diagnosis. According to the St Jude’s staging system, eligible patients had stage II, III, or IV disease. Patients with disease isolated to the skin, stage I disease, or central nervous system involvement were not eligible. Additional exclusion criteria included previous cytotoxic chemotherapy, known immunodeficiency, organ transplant recipient, pregnant female, known HIV+ status, and weight <10 kg. Previous steroid treatment and/or radiation treatment was not allowed unless it was for the emergent management of a mediastinal mass. In addition, patients chronically receiving medications known to be metabolized by CYP3A4 with narrow therapeutic indices were not eligible because of drug interaction with the 2 investigational agents. All patients underwent a physical examination, computed tomography scans, complete blood count, biochemical profile, bone marrow examination, cerebrospinal fluid examination, and assessment of lactate dehydrogenase level to determine the extent of disease. A positron emission tomography scan with 2-deoxy-2-[fluorine-18]fluoro-d-glucose could be used for disease evaluation but was not mandated by the study.
Treatment protocol
Eligible patients received chemotherapy based on the protocol used in the International ALCL99 Trial (ALCL99), which is the largest clinical trial for pediatric ALCL. It is considered the standard of care, when using the ALCL99 regimen for the treatment of ALCL, to use 3 g/m2 of methotrexate over 3 hours and to give a single dose of intrathecal chemotherapy during prophase, with no other intrathecal chemotherapy.10 All patients received 5-day prophase, followed by 6 alternating cycles administered every 21 days (Table 2). The treatment duration was 5 months. No patient received radiation. Growth factors were not mandated on the study but could be used at the treating institution’s discretion.
Chemotherapy schedule
| Course | Drug | Daily dose | Schedule |
|---|---|---|---|
| Prophase (days 1-5) | Cyclophosphamide | 200 mg/m2 | Days 1 and 2 |
| Dexamethasone | 5 mg/m2 | Days 1 and 2 | |
| 10 mg/m2 | Days 3-5 | ||
| Triple intrathecal | Age based | Day 1 | |
| Cycles 1, 3, and 5 | Brentuximab vedotin* | 1.8 mg/kg | Day 1 |
| Methotrexate | 3 g/m2 over 3 h | Day 1 | |
| Dexamethasone | 10 mg/m2 | Days 1-5 | |
| Ifosfamide | 800 mg/m2 | Days 1-5 | |
| Etoposide | 100 mg/m2 | Days 4 and 5 | |
| Cytarabine | 150 mg/m2 × 2 | Days 4 and 5 | |
| Cycles 2, 4, and 6 | Brentuximab vedotin* | 1.8 mg/kg | Day 1 |
| Methotrexate | 3 g/m2 over 3 h | Day 1 | |
| Dexamethasone | 10 mg/m2 | Days 1-5 | |
| Cyclophosphamide | 200 mg/m2 | Day 1-5 | |
| Doxorubicin | 25 mg/m2 | Days 4 and 5 |
| Course | Drug | Daily dose | Schedule |
|---|---|---|---|
| Prophase (days 1-5) | Cyclophosphamide | 200 mg/m2 | Days 1 and 2 |
| Dexamethasone | 5 mg/m2 | Days 1 and 2 | |
| 10 mg/m2 | Days 3-5 | ||
| Triple intrathecal | Age based | Day 1 | |
| Cycles 1, 3, and 5 | Brentuximab vedotin* | 1.8 mg/kg | Day 1 |
| Methotrexate | 3 g/m2 over 3 h | Day 1 | |
| Dexamethasone | 10 mg/m2 | Days 1-5 | |
| Ifosfamide | 800 mg/m2 | Days 1-5 | |
| Etoposide | 100 mg/m2 | Days 4 and 5 | |
| Cytarabine | 150 mg/m2 × 2 | Days 4 and 5 | |
| Cycles 2, 4, and 6 | Brentuximab vedotin* | 1.8 mg/kg | Day 1 |
| Methotrexate | 3 g/m2 over 3 h | Day 1 | |
| Dexamethasone | 10 mg/m2 | Days 1-5 | |
| Cyclophosphamide | 200 mg/m2 | Day 1-5 | |
| Doxorubicin | 25 mg/m2 | Days 4 and 5 |
Brentuximab vedotin was given prior to any other chemotherapy on day 1.
Brentuximab vedotin was administered on day 1 of each of the 6 cycles for a total of 6 doses. The starting dose of brentuximab vedotin was 1.8 mg/kg (maximum dose, 180 mg) given IV over 30 minutes on day 1 of each cycle prior to all other chemotherapy. Dose reductions to 1.2 mg/kg (maximum dose, 120 mg), followed by 0.8 mg/kg (maximum dose, 80 mg), were mandated for certain toxicities. Any grade of anaphylaxis or progressive multifocal leukoencephalopathy, grade 3 or 4 pancreatitis, grade 4 peripheral neuropathy, or grade 3 or 4 pneumonitis that was probably or definitely related to brentuximab vedotin required permanent discontinuation of brentuximab vedotin. Severe renal impairment (creatinine clearance <30 mL/min) for any reason required discontinuation of brentuximab vedotin. Grade 2 pancreatitis, grade 2 or 3 peripheral neuropathy, grade 2 pneumonitis, or grade 3 or 4 nonhematologic events (with the exception of electrolyte abnormalities and those specifically mentioned) that were probably or definitely related to brentuximab vedotin required dose reduction. Amendment 2 changed the requirement for a dose reduction secondary to mucositis from grade 3 or 4 to only grade 4. Patients who were unable to begin a cycle within 35 days from the start of the previous cycle (>14-day delay) because of neutropenia with no other dose-limiting toxicity received the same dose of brentuximab vedotin in the next cycle with myeloid growth factor support if not used. Patients who were unable to begin a cycle within 35 days from the start of the previous cycle (>4-day delay) even with myeloid growth factor support, because of neutropenia with no other dose-limiting toxicity, required dose reduction of brentuximab vedotin.
Patients were evaluated for response after cycle 2 and cycle 6. A cycle-4 evaluation was performed on patients who did not achieve a complete response after cycle 2. Complete response was defined as disappearance of all evidence of disease. Complete response, unconfirmed was defined as a residual lymph node mass >1.5 cm that regressed by >75% in the sum of the products of the greatest perpendicular diameters or returned to normal size or any residual lesion in organs that decreased by >75% with a negative positron emission tomography scan. Partial response was defined as >50% decrease in the sum of the products of the greatest perpendicular diameters of the lesions with no new lesions. Patients were declared off protocol therapy if they developed progressive disease at any time. After completion of therapy, follow-up was performed every 3 months for the first year, every 6 months during years 2 and 3, and then yearly. All relapses were to be confirmed by biopsy.
Toxicity assessment
Adverse events and clinically significant laboratory findings were collected using NCI Common Terminology Criteria for Adverse Events Version 4.0. Additional reporting was done through the NCI Adverse Event Expedited Reporting System. Required reporting included all grade 3+ nonhematological nontargeted toxicities, all grade 2+ thromboembolic events, and all hematologic and nonhematologic toxicities that resulted in hospitalization or delay in therapy. Patients were monitored weekly during therapy for hematological toxicities and clinical side effects. Serum chemistries, including aspartate aminotransferase, alanine aminotransferase, and bilirubin, were obtained weekly during cycles 1 and 2 and then at the start of each cycle. An echocardiogram and electrocardiogram were obtained prior to each dose of doxorubicin.
Pathology
Institutional phenotyping (by flow cytometry or immunohistochemical staining) was required as a part of the confirmation of the diagnosis. Recommended antibodies to determine diagnosis included 2 anti-B antibodies (CD79A and CD20), 2 anti-T antibodies (CD3 and CD43 or CD3 and CD45RO), CD30, CD15, EMA, ALK-1, and LMP-1 or EBER. All cases were required to be positive for CD30 and ALK. ALK positivity was determined at the institutional level by immunohistochemical staining or fluorescence in situ hybridization.
Correlative biology studies
In patients with ALCL, serial assessments of the t(2;5)(p23;q35) NPM-ALK fusion transcript were evaluated in 1 laboratory by quantitative reverse transcription polymerase chain reaction (qRT-PCR). Although the specific cellular localization of ALK was not captured, based on the frequency of NPM-ALK rearrangements, which represent ∼85% to 90% of ALK+ ALCLs in the pediatric population,24 we focused on assessment of the NPM-ALK fusion transcripts for the analysis of minimal disseminated disease (MDD). Baseline peripheral blood samples were obtained, as were blood samples on day 1 of cycle 1 and day 1 of cycle 2. Peripheral blood was collected in EDTA tubes and shipped overnight, within 24 hours of being collected, to a central laboratory for analysis. qRT-PCR was performed by extracting total RNA from bone marrow and peripheral blood specimens. The normalized copy numbers (NCNs) were expressed as copy numbers of NPM-ALK per 104 copies of ABL, as previously published.25 MDD is defined as >10 NCNs at baseline.
Statistical analysis
The primary study end points were the occurrence of grade 3+ nonhematologic adverse events and EFS. All patients assigned to arm BV who received protocol therapy (including those that only received prophase therapy) contributed to the primary EFS analysis. EFS was defined as the time from study entry until disease progression, relapse, or death. Patients who did not experience an EFS event were censored at the last date of contact. Only patients who received ≥1 dose of brentuximab vedotin contributed to the toxicity analysis.
The study chair reviewed reported toxicities on a weekly basis. All deaths and patients removed from the study as a result of toxicity were reported to the data and safety monitoring committee for review. The study committee had conference calls at least every month, reviewing all of the adverse experience data. Because of the initial concern regarding pulmonary toxicity with brentuximab vedotin,26 this toxicity was specifically monitored. Interim analysis of this rate was performed with an exact binomial rule, using 5% as an acceptable toxicity rate and 15% as an unacceptable rate, with a 4% chance of declaring a 5% rate unacceptable and an 86% chance of declaring a 15% rate unacceptable. Interim analysis of these rates was performed using an α-spending function approach and an O’Brien-Fleming monitoring boundary (truncated at 3 standard deviations) with 3 planned interim analyses. The actual interim analyses took place at 39% (25 patients), 58% (37 patients), and 72% (46 patients) of expected information.
EFS was compared with a historical control cure model with a “cure” rate of 70% and exponential failures with exponent 1.5. A sample size of 64 eligible patients would provide the study with 90% power to detect a hazard ratio of 0.5 (“cure” rate improved to 84%) using the log-rank test at a 1-sided significance level of 0.10. Accrual was planned for 68 patients to ensure 64 eligible patients. The study was not designed or powered to compare arm BV with arm CZ.
Patient characteristics and toxicities were summarized as frequencies and percentages. EFS and OS distributions were estimated using the Kaplan-Meier method. A comparison of time-to-event distributions was made using the log-rank test. Univariate analysis of prognostic factors of EFS and OS was conducted using Cox regression for variables that occurred in at least 10% of patients. P values <.05 were considered statistically significant. SAS software version 9.2 (SAS Institute Inc, Cary, NC) was used for data analysis.
Results
Patient characteristics
ANHL12P1 enrolled 68 patients on arm BV between 8 November 2013 and 20 January 2017. The 68 patients were enrolled at 52 separate COG sites. Data as of 30 September 2019 are included in this report. Forty-eight patients were randomized to arm BV, and 20 patients were nonrandomly assigned to arm BV because of body surface area <0.9 m2; all 68 are included in the outcome analysis. One patient was taken off protocol at the treating physician’s discretion during prophase before receiving brentuximab vedotin, leaving 67 eligible patients for toxicity evaluation. Baseline characteristics are listed in Table 3. Median age at enrollment was 12 years (range, 2-21). There were 43 males (63.2%) and 25 females (36.8%) on arm BV. Extranodal sites of disease were common, with 42 patients (61.8%) having ≥1 site.
Clinical characteristics of 68 children with ALCL
| Characteristic | N (%) |
|---|---|
| Age, y | |
| Median | 12 |
| Range | 2-21 |
| Age group, y | |
| <6 | 13 (19.1) |
| 6-12 | 25 (36.8) |
| ≥13 | 30 (44.1) |
| Sex | |
| Male | 43 (63.2) |
| Female | 25 (36.8) |
| Race | |
| White | 48 (70.6) |
| Black or African American | 8 (11.8) |
| Asian | 5 (7.3) |
| American Indian or Alaska Native | 1 (1.5) |
| Multiple races | 1 (1.5) |
| Unknown or not reported | 5 (7.3) |
| Ethnicity | |
| Hispanic or Latino | 5 (7.4) |
| Not Hispanic or Latino | 60 (88.2) |
| Unknown or not reported | 3 (4.4) |
| Stage | |
| Stage II | 11 (16.2) |
| Stage III | 48 (70.6) |
| Stage IV | 9 (13.2) |
| Site of disease | |
| Lymph node | 65 (95.6) |
| Bone | 16 (23.5) |
| Bone marrow | 9 (13.2) |
| Liver | 1 (1.5) |
| Lung | 9 (13.2) |
| Skin | 3 (4.4) |
| Soft tissue | 20 (29.4) |
| Spleen | 7 (10.3) |
| Characteristic | N (%) |
|---|---|
| Age, y | |
| Median | 12 |
| Range | 2-21 |
| Age group, y | |
| <6 | 13 (19.1) |
| 6-12 | 25 (36.8) |
| ≥13 | 30 (44.1) |
| Sex | |
| Male | 43 (63.2) |
| Female | 25 (36.8) |
| Race | |
| White | 48 (70.6) |
| Black or African American | 8 (11.8) |
| Asian | 5 (7.3) |
| American Indian or Alaska Native | 1 (1.5) |
| Multiple races | 1 (1.5) |
| Unknown or not reported | 5 (7.3) |
| Ethnicity | |
| Hispanic or Latino | 5 (7.4) |
| Not Hispanic or Latino | 60 (88.2) |
| Unknown or not reported | 3 (4.4) |
| Stage | |
| Stage II | 11 (16.2) |
| Stage III | 48 (70.6) |
| Stage IV | 9 (13.2) |
| Site of disease | |
| Lymph node | 65 (95.6) |
| Bone | 16 (23.5) |
| Bone marrow | 9 (13.2) |
| Liver | 1 (1.5) |
| Lung | 9 (13.2) |
| Skin | 3 (4.4) |
| Soft tissue | 20 (29.4) |
| Spleen | 7 (10.3) |
Treatment
Overall, 67 of 68 (99%) patients received ≥1 dose of brentuximab vedotin. Sixty-three of 67 (94%) patients received all 6 planned doses of brentuximab vedotin without dose modification. Of the 3 patients who received a reduced dose of brentuximab vedotin, 1 patient received doses of 1.2 mg/kg during cycles 5 and 6 because of mucositis during cycle 4, 1 patient received doses of 1.2 mg/kg during cycles 3 through 6 because of mucositis during cycle 2, and 1 patient received doses of 1.2 mg/kg during cycles 2 and 3 because of elevated alanine aminotransferase during cycle 1. The last patient was taken off protocol after cycle 3 at the treating physician’s discretion. None of the 3 patients who required a dose reduction required a second dose reduction. Growth factor was given in 207 of 399 (51.9%) cycles.
One patient was taken off protocol at the treating physician’s discretion during prophase before receiving brentuximab vedotin, leaving 67 eligible patients for toxicity evaluation. Sixty-six of 67 patients completed all 6 cycles of chemotherapy, resulting in 399 cycles evaluable. Toxicity results are listed in Table 4. There were no toxic deaths, no case of progressive multifocal leukoencephalopathy syndrome, and no case of grade 3 or 4 neuropathy. Grade 3 or 4 toxicities that occurred in >5% of cycles included hematological toxicities, mucositis, and febrile neutropenia. The mean/median interval between each cycle was: 22.7/22 days (cycle 1 to 2), 22.7/21 days (cycle 2 to 3), 22.8/21 days (cycle 3 to 4), 23.0/21 days (cycle 4 to 5), and 22.8/21 days (cycle 5 to 6). The interval between cycles was >28 days (>1-week delay) in only 3.6% of all cycles.
Grade 3 and 4 toxicities experienced on arm BV of ANHL12P1 (399 cycles)
| Grade 3 | Grade 4 | |||
|---|---|---|---|---|
| Adverse event | No. of cycles | % | No. of cycles | % |
| Hematological | ||||
| Anemia | 55 | 13.8 | 3 | 0.8 |
| Neutropenia | 20 | 5.0 | 76 | 19.0 |
| Thrombocytopenia | 22 | 5.5 | 34 | 8.5 |
| Febrile neutropenia | 52 | 13.0 | 2 | 0.5 |
| Gastrointestinal | ||||
| Mucositis oral | 21 | 5.3 | 1 | 0.3 |
| Anaphylaxis | 1 | 0.3 | ||
| Infections | ||||
| Appendicitis | 1 | 0.3 | ||
| Catheter-related infection | 2 | 0.5 | ||
| Infections and infestations; other, specify | 7 | 1.8 | 1 | 0.3 |
| Lung infection | 3 | 0.8 | ||
| Sepsis | 1 | 0.3 | ||
| Skin infection | 1 | 0.3 | ||
| Urinary tract infection | 2 | 0.5 | ||
| Laboratory | ||||
| Alanine aminotransferase increased | 15 | 3.8 | 4 | 1.0 |
| Aspartate aminotransferase increased | 8 | 2.0 | 1 | 0.3 |
| Hypokalemia | 13 | 3.3 | 1 | 0.3 |
| Vascular | ||||
| Thromboembolic event | 3 | 0.8 | ||
| Grade 3 | Grade 4 | |||
|---|---|---|---|---|
| Adverse event | No. of cycles | % | No. of cycles | % |
| Hematological | ||||
| Anemia | 55 | 13.8 | 3 | 0.8 |
| Neutropenia | 20 | 5.0 | 76 | 19.0 |
| Thrombocytopenia | 22 | 5.5 | 34 | 8.5 |
| Febrile neutropenia | 52 | 13.0 | 2 | 0.5 |
| Gastrointestinal | ||||
| Mucositis oral | 21 | 5.3 | 1 | 0.3 |
| Anaphylaxis | 1 | 0.3 | ||
| Infections | ||||
| Appendicitis | 1 | 0.3 | ||
| Catheter-related infection | 2 | 0.5 | ||
| Infections and infestations; other, specify | 7 | 1.8 | 1 | 0.3 |
| Lung infection | 3 | 0.8 | ||
| Sepsis | 1 | 0.3 | ||
| Skin infection | 1 | 0.3 | ||
| Urinary tract infection | 2 | 0.5 | ||
| Laboratory | ||||
| Alanine aminotransferase increased | 15 | 3.8 | 4 | 1.0 |
| Aspartate aminotransferase increased | 8 | 2.0 | 1 | 0.3 |
| Hypokalemia | 13 | 3.3 | 1 | 0.3 |
| Vascular | ||||
| Thromboembolic event | 3 | 0.8 | ||
CTCAE, Common Terminology Criteria for Adverse Events version 4.0.
Outcome
Fourteen patients relapsed, and these were the only events contributing to EFS. Fifty-four patients did not experience an event and were censored at their last date of contact. All of the events occurred within 2 years of the patient’s enrollment date. Relapses were confirmed by biopsy in all 14 cases, with 11 (79%) occurring within 10 months of initial diagnosis. Median time from diagnosis to relapse was 7.5 months (range, 5.5-22). Only 1 of 68 patients (1.5%) relapsed prior to off-therapy evaluation. This relapse occurred 5.5 months from diagnosis after the sixth cycle of chemotherapy was completed, but before off-therapy evaluations were performed. There were no relapses that involved the central nervous system. The 2-year EFS estimate is 79.1% (95% confidence interval [CI], 67.2-87.1). The 2-year OS is 97.0% (95% CI, 88.1-99.2). The median follow-up for patients alive at last contact was 2.5 years (range, 1.2-5.2).
The complete response rate (complete response + complete response, unconfirmed) for patients who underwent evaluation was 62% after cycle 2 (41/66 patients) and 97% after cycle 6 (62/64 patients). As discussed previously, 2 patients were removed from the protocol at the treating physician’s discretion, 1 patient relapsed immediately prior to cycle 6 evaluation, and 1 patient was not assessed.
Prognostic factors
Prognostic factors of EFS were evaluated for the entire cohort of patients using univariate analysis. Only lung involvement was associated with EFS (age, P = .35; sex, P = .067; ethnicity, P = .83; stage, P = .13; bone involvement, P = .11; bone marrow involvement, P = .2; lung, P = .026; soft tissue involvement, P = .45); spleen, P = .053; supplemental Table 1, available on the Blood Web site).
MDD measured in peripheral blood by qRT-PCR and utilizing >10 NCNs as positive was highly predictive of outcome. Of the 68 patients assigned to arm BV, 57 patients had available baseline data and were included in the analyses. The missing 11 samples represent those that were not received (n = 4) or samples of inadequate RNA quality (n = 7). The 2-year EFS estimate is 89.0% (95% CI, 73.1-95.7) for MDD-negative cases (n = 38) and 52.6% (95% CI, 28.7- 71.9 for MDD-positive cases (n = 19). The estimated EFS and OS distributions by MDD are presented in Figures 1 and 2.
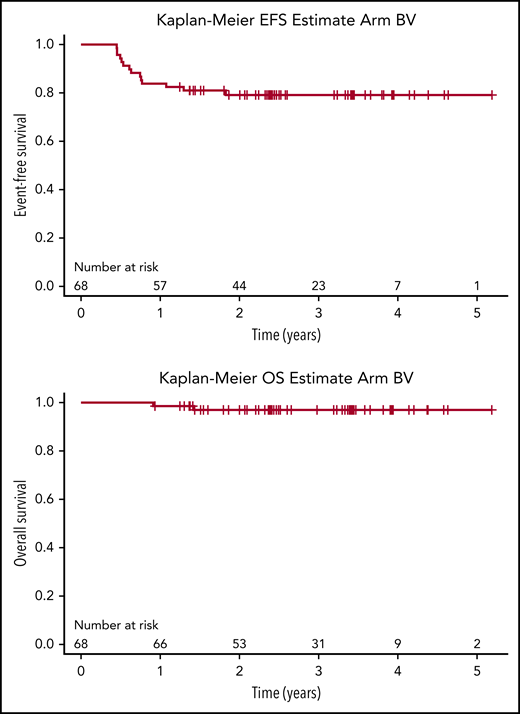
EFS (2-year, 79.1%; 95% CI, 67.2-87.1) and OS (2-year, 97%; 95% CI, 88.1-99.2) for newly diagnosed patients with ALK+ ALCL in arm BV of ANHL12P1.
EFS (2-year, 79.1%; 95% CI, 67.2-87.1) and OS (2-year, 97%; 95% CI, 88.1-99.2) for newly diagnosed patients with ALK+ ALCL in arm BV of ANHL12P1.
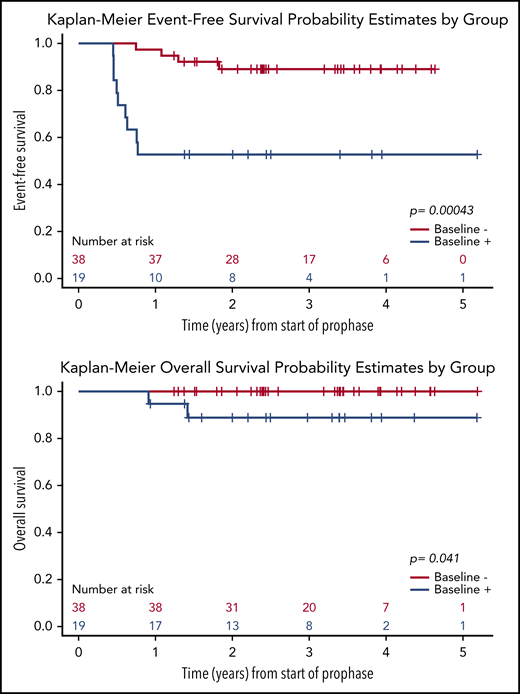
EFS and OS of newly diagnosed patients with ALK+ALCL in arm BV of ANHL12P1, according to baseline MDD (n = 57; MDD negative = 38, MDD positive = 19). qRT-PCR with a cutoff >10 copies of NPM-ALK per 104 copies of ABL was used to define MDD positivity.
EFS and OS of newly diagnosed patients with ALK+ALCL in arm BV of ANHL12P1, according to baseline MDD (n = 57; MDD negative = 38, MDD positive = 19). qRT-PCR with a cutoff >10 copies of NPM-ALK per 104 copies of ABL was used to define MDD positivity.
Discussion
Different strategies for treating children with ALCL have emerged with similar success rates (Table 1). The reason for the variation in treatment strategies is multifactorial. Initially, clinical trials for ALCL used different treatment strategies, because there was no standard of care for this rare disease. Because these various strategies resulted in similar outcomes, subsequent cooperative group trials attempted to intensify treatment based on their preferred strategy. None of the intensified treatment strategies resulted in an improvement in the survival of pediatric patients with ALCL.8,12-14 Fortunately, targeted agents with excellent activity against ALCL, such as brentuximab vedotin,21 have emerged and been shown to improve progression-free survival in adults with ALCL,27 offering renewed hope that the survival of patients with ALCL can be improved.
This report describes the results of adding brentuximab vedotin to standard chemotherapy. Overall outcomes were favorable with a 2-year EFS of 79.1% (95% CI, 67.2-87.1) and a 2-year OS of 97% (95% CI, 88.1-99.2). This trial replicated the inclusion and exclusion criteria (with the exception of nonresected stage I patients) and the chemotherapy dosing and schedule (with the exception of brentuximab vedotin) of ALCL99 to provide a comparison that was as close to historical data as possible (Table 1).
Like previous pediatric ALCL trials, the vast majority of relapses occurred shortly after the completion of chemotherapy. The mean time to relapse from initiation of chemotherapy was 7.5 months in this study compared with 6.5 months in the vinblastine-free arm of ALCL99.12 Importantly, however, there were no progressions or relapses in the current study while receiving therapy, with the earliest occurring 5.5 months from diagnosis, suggesting that brentuximab vedotin was an extremely effective agent at preventing relapse. This is the first clinical trial in which no patient progressed or experienced disease recurrence while receiving therapy. This finding is important because patients who relapse/progress during treatment have the poorest outcome.18,28 A more recent study of 17 children with ALCL, who progressed at a median of 3.7 months from initial diagnosis, demonstrated an EFS of 41% when scheduled to receive an allogenic stem cell transplant.19 Of note, the impact of brentuximab vedotin on the high OS observed in the current study will be difficult to discern because recent studies produced a high OS,29 and relapsed patients also likely benefited from the current availability and success of ALK inhibitors in treating relapsed ALCL.30-32
Despite the activity of vinblastine in ALCL, its addition to chemotherapy has not resulted in an improvement in survival. ALCL99 showed that addition of vinblastine as maintenance therapy did not improve the 2-year EFS for patients with newly diagnosed ALCL.12 The ANHL0131 study showed that the addition of weekly vinblastine to the APO (doxorubicin, prednisone, vincristine, methotrexate, 6‐mercaptopurine) chemotherapy backbone also did not improve EFS and was associated with an increased incidence of toxicity.8 Although the antineoplastic activity of vinblastine and brentuximab vedotin is an antitubulin agent, it is possible that brentuximab vedotin prevented relapses during therapy as a result of its ability to target ALCL cells through CD30. Preclinical data demonstrated that MMAE binds to a similar site on tubulin as does vinblastine.33 Using a CD30+ cell line, Alley et al demonstrated that brentuximab vedotin had a peak tumor concentration that was 10- to 30-fold greater than MMAE or vinblastine delivered in a nontargeted fashion.34 In addition, over 3 days, the tumor exposure to MMAE after brentuximab vedotin was fivefold to 10-fold higher than when given as a nontargeted agent.
Two major concerns related to adding new agents to standard chemotherapy are an increased incidence of toxicity and an inability to administer the standard chemotherapy as desired. The addition of brentuximab vedotin to standard chemotherapy did not add significant toxicity compared with the toxicities observed on the ALCL99 protocol.35 The grade 3/4 toxicity rates on ALCL99 (2050 courses) were similar to the current study (399 courses) (mucositis, 13% vs 5%, respectively; increased AST/alanine aminotransferase, 10% to 7%; infection, ∼5% vs 5%; and neuropathy, <1% on both). Interestingly, there was no case of peripheral neuropathy during our study, which is in direct contrast to the experience in adult patients; peripheral neuropathy is a common adverse event associated with exposure to brentuximab vedotin.21 It may be that younger age was protective against this particular side effect and/or 6 doses did not reach the cumulative dose necessary to cause neuropathy. The higher rate of hematological toxicity in ALCL99 compared with our study is likely secondary to the widespread use of growth factors in our study, as well as the different guidelines used for transfusion of red cells and platelets across clinical trial groups. Brentuximab vedotin did not change the desired interval between cycles and was given at the full dose in 94% of patients, despite strict dose-reduction criteria.
Several groups have established the prognostic significance of qualitative and quantitative detection of MDD in bone marrow and blood mononuclear cells. Our study specifically collected peripheral blood to measure MDD because it was the least invasive procedure and was most likely to be obtained in future international collaborative trials. In previous studies using qualitative detection, 50% to 60% of patients were MDD-positive with a risk for relapse ∼50% compared with 15% for MDD-negative patients.25 Quantification of MDD has been shown by 1 group to have even greater prognostic significance. Damm-Welk et al demonstrated that patients with >10 NCNs of NPM-ALK circulating in peripheral blood had a cumulative incidence of relapse of 59% (n = 17; 24% of patients) compared with 15% (n = 53; 76% of patients) in patients with NCNs below that threshold.36 The results of the current trial showed a similar distribution to that study, with 19 (33%) of patients being MDD-positive with an EFS of 52%. Our results and the distribution of MDD-positive patients were similar to a Japanese study in which patients were treated using ALCL99 without brentuximab vedotin; EFS was 57.8% in MDD-positive patients (n = 22; 37%) and 84.9% in MDD-negative patients (n = 37; 63%).37 The differences between the studies are likely secondary to the small number of patients, the combined use of bone marrow and peripheral blood, inclusion or exclusion of translocations other than NPM-ALK, and methods used to determine MDD quantification. Importantly, as a result of interlaboratory differences, the reproducibility of qRT-PCR for NPM-ALK has not been demonstrated, making direct comparisons imperfect. Regardless, our study has reaffirmed the potential use of MDD in peripheral blood to establish risk categories and the need for quantitative MDD analysis to be harmonized across research groups in the future.
Although ALCL is a rare subtype of lymphoma, the COG was able to enroll 68 patients across 52 sites. Only through broad cooperation could a trial such as this occur. Unfortunately, having multiple sites, each with few patients, makes it difficult to coordinate definitive pathological subtyping of disease. Five histological subtypes are recognized within ALK+ ALCL: common histology, lymphohistiocytic, small cell, Hodgkin-like pattern, and composite pattern. Although variant subtypes have prognostic implications, concordance in identifying subtype variants among pathologists is lower than with many other lymphomas.38 Thus, ANHL12P1 is unable to test the effect of brentuximab vedotin on individual subtypes because we are unable to classify each case with certainty.
In summary, arm BV of ANHL12P1 demonstrated that the addition of brentuximab vedotin prevented relapses during therapy and resulted in efficacy at least as good as with previously reported regimens used to treat children with nonlocalized ALCL. The study further demonstrated that brentuximab vedotin did not increase toxicity and was feasible to give in a 21-day cycle. The study confirmed that MDD detection in peripheral blood was prognostic, with a significant impact on EFS. Lastly, the study demonstrated that a clinical trial using a targeted agent in newly diagnosed patients with a rare cancer is possible. Continued collaboration among cooperative trial groups is critical to define the optimal strategy for incorporating brentuximab vedotin into therapy for patients with ALCL, especially those at high risk for relapse.
Data sharing requests should be sent to Eric J. Lowe (eric.lowe@chkd.org).
The online version of this article contains a data supplement.
The publication costs of this article were defrayed in part by page charge payment. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
There is a Blood Commentary on this article in this issue.
Acknowledgments
This work was supported by the National Institutes of Health, National Cancer Institute’s National Clinical Trial Network (NCTN) Operations Center grant U10CA180886 and NCTN Statistics and Data Center grant U10CA180899); and by the St Baldrick’s Foundation.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Authorship
Contribution: E.J.L. conceived and designed the clinical trial, performed research, and analyzed data; A.F.R. designed and performed research; M.S.L. coordinated pathology and designed MDD research; T.G.G. designed research; L.S. and D.A.B. analyzed and interpreted data and performed statistical analyses; M.S.L. and R.W. performed MDD research; S.A. interpreted data; C.M.B. designed research and led the group; T.G.G., S.A., and C.M.B. provided insightful views and critiques; and A.F.R., M.S.L., T.G.G., D.A.B., R.W., S.A., and C.M.B. edited the manuscript.
Conflict-of-interest disclosure: M.S.L. is on the Advisory Board for Seattle-Genetics. D.A.B.’s spouse is employed by Genentech. The remaining authors declare no competing financial interests.
Correspondence: Eric J. Lowe, Department of Pediatric Hematology/Oncology, Children’s Hospital of the King’s Daughters, 601 Children’s Lane, Norfolk, VA 23507; e-mail: eric.lowe@chkd.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal