


Viktoria Blumenberg and Maria-Luisa Schubert contributed equally.
Introduction: The CD19 specific chimeric antigen receptor (CAR) T-cell products Axicabtagene-Ciloleucel and Tisagenlecleucel are approved for the treatment of refractory/relapsed B-cell precursor ALL (BCP-ALL) and Diffuse Large B-cell lymphoma (DLBCL). Despite high response rates, long term remission is only achieved in a subgroup if patients. In addition, CAR T cell therapy is accompanied by potentially severe immune related toxicities including cytokine release syndrome (CRS) or neurotoxicity (ICANS). Therefore, we need to identify biological mechanisms of treatment resistance and toxicity occurring in the host in addition to improve the CAR T product itself. The impact of the gut microbiome on T-cell based immunotherapies such as checkpoint inhibition or allogeneic hematopoietic stem cell transplant has been shown, but it´s role in mediating anti-tumor responses and the occurrence of immunotoxicities of CAR T-cell therapy has not yet been reported so far.
Methods: Patients with r/r BCP-ALL and DLBCL were treated with the commercially available CD19 specific CAR T-cell products Axicabtagene-Ciloleucel or Tisagenlecleucel or in-house manufactured CD19-targeted CD28-4-1BB-CD3ζ CAR T-cells at both our institutions. Fecal biospecimens from 33 patients were collected sequentially before, during and after CAR T transfusion (specific time points: before lymphodepleting chemotherapy, day of CAR T-cell transfusion and in 7 day intervals up to day 28). 16S rRNA sequencing and shotgun metagenome sequencing has been performed on 137 stool samples. Sequencing results and clinical metadata are integrated into a patient-centered "hospitalome" including infections and immunotoxicities as well as concomitant anti-infective, immunosuppressive agents and treatment response. Patients having received any type of anti-infective medication exceeding prophylaxis on the day of CAR T cell transfusion or up to two weeks prior were distinguished from patients without prior anti-infective medication or only receiving anti-infective drugs from day 1 after CAR T-cell transfusion.
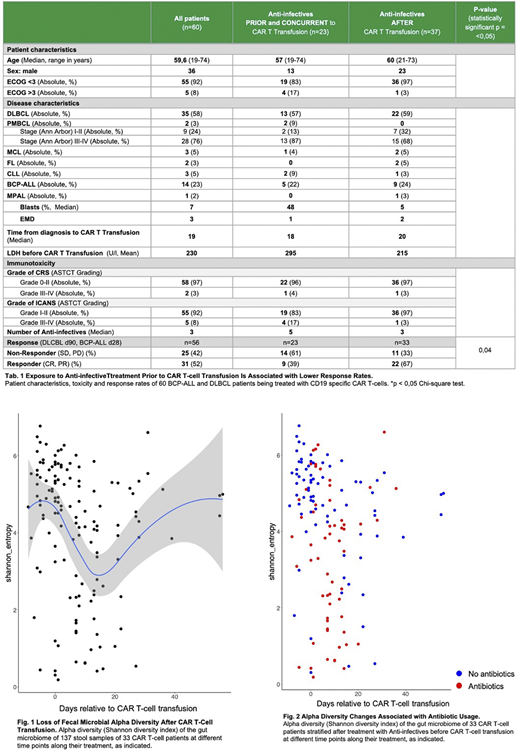
Results: Patients receiving anti-infectives up to two weeks prior to CAR T-cell transfusion display a significantly lower response rate compared to patients, who have been treated with antibiotic and / or -mycotic treatment after day 0 (Tab. 1). Before CAR T-cell transfusion patients showed a heterogeneous, but largely diverse gut microbial taxa (Shannon index median: 4.2.). After CAR T-cell transfusion the alpha diversity (i.e. within-sample diversity) decreases with the nadir at day 14 (Shannon index, median 2.4), which depended significantly on broad-spectrum antibiotic administration (Fig. 1-2). Furthermore, loss of diversity correlated significantly with the occurrence of CRS (p<0.001, univariate GLM with Shannon diversity index vs. occurrence of CRS, irrespective of grade). Diversity loss was not associated with clinical response at day 90 or the development of ICANS. Age had no effect on microbiome changes and no inter-center effect was detected. Assessment of beta diversity (i.e. variation between samples) demonstrated compositional changes of the microbiome in CAR T-cell patients with approximately 25% of all samples displaying a mono-domination of the microbiome by Enterococcus spp. (i.e., rel. abundance > 30% per sample). The expansion of enterococci was again found in samples of patients, who received antibiotic treatment.
Conclusion: The gut microbiome of CAR T-cell patients undergoes large and diverse compositional changes, whereas altered diversity is significantly associated with administration of anti-infectives prior to CAR T-cell transfusion and the occurrence of CRS. The assessment of the gut microbial taxa of CAR T-cell patients might serve as a predictive biomarker for immunotoxicity and, eventually, treatment response.
Blumenberg:Gilead: Consultancy, Research Funding; Novartis: Research Funding; Celgene: Research Funding. Schubert:Kite / Gilead: Consultancy; Takeda: Consultancy. Buecklein:Amgen: Consultancy; Pfizer: Consultancy; Celgene: Research Funding; Novartis: Research Funding; Gilead: Consultancy, Research Funding. Müller-Tidow:Pfizer: Research Funding, Speakers Bureau; Daiichi Sankyo: Research Funding; BiolineRx: Research Funding; Janssen-Cilag GmbH: Speakers Bureau. Dreger:Gilead: Consultancy, Speakers Bureau; AbbVie: Consultancy, Speakers Bureau; AstraZeneca: Consultancy; Roche: Consultancy, Speakers Bureau; Neovii: Research Funding; Riemser: Consultancy, Research Funding, Speakers Bureau; Janssen: Consultancy; Novartis: Consultancy, Speakers Bureau. Schmitt:Apogenix: Research Funding; Hexal: Other: Travel grants , Research Funding; Novartis: Other: educational activities and conferences, Research Funding; Kite: Other: Travel grants, educational activities and conferences; MSD: Membership on an entity's Board of Directors or advisory committees, Other: PI of clinical trials on letermovir; TolerogenixX Ltd: Other: Co-Founder and shareholder. Subklewe:Roche AG: Consultancy, Research Funding; Novartis: Consultancy, Research Funding; AMGEN: Consultancy, Honoraria, Research Funding; Janssen: Consultancy; Pfizer: Consultancy, Honoraria; Gilead Sciences: Consultancy, Honoraria, Research Funding; Seattle Genetics: Research Funding; Morphosys: Research Funding; Celgene: Consultancy, Honoraria.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal