

TO THE EDITOR
Transfusion of COVID-19 convalescent plasma (CCP) as a means to reduce the severity of the disease and help resolve the infection more rapidly is currently being investigated in more than 100 clinical trials. The beneficial effects of CCP transfusion in COVID-19 patients were recently reported, although most of the studies were not randomized controlled trials or they involved only a few patients.1-7 One of the main hypotheses to explain the potential clinical benefits of CCP is the presence of SARS-CoV-2–neutralizing antibodies (nAbs).8,9 Consequently, several groups have included nAb titers as a criterion for the selection of CCP units to be transfused.10,11 A good correlation between nAb and SARS-CoV-2 spike protein receptor binding domain (RBD) antibody titers has been reported,11-14 and therefore analysis of SARS-CoV-2 spike RBD antibodies using enzyme-linked immunosorbent assay (ELISA) represents a valuable tool for the initial characterization of CCP.
Héma-Québec, the agency responsible for the blood supply in Quebec, Canada, is involved in the collection and testing of CCP used in a randomized open-label trial of Convalescent Plasma for Hospitalized Adults with Acute COVID-19 Respiratory Illness (CONCOR-1, clinicaltrials.gov identifier #NCT04348656) designed to determine the effect of CCP at reducing the risk of intubation or death in adult patients hospitalized for COVID-19. Potential donors were recruited after at least 14 days of resolution of COVID-19 symptoms (see supplemental Methods for additional information, available on the Blood Web site). Initial diagnosis had been confirmed by public health authorities through either polymerase chain reaction or epidemiologic contact. All participants met the donor selection criteria for plasma donation in use at Héma-Québec and consented to the study. Seropositivity (presence of antibodies against SARS-CoV-2 RBD) was determined using a semiquantitative ELISA (supplemental Methods) adapted from previous work.15,16 Consistent with previous reports on the rate of seroconversion of COVID-19 patients,17-19 the overall proportion of our convalescent plasma donors (n = 282) that were tested seronegative at the time of donation was 6.9%. However, this proportion increased to about 15% when considering only donors who had waited for more than 11 to 12 weeks after symptom onset before donating (supplemental Table). This prompted us to perform a longitudinal analysis of the anti-RBD antibody response in CCP donors (11 males and 4 females; median age, 56 years; range, 20-67 years) who donated at least 4 times, during a time interval after symptom onset ranging from 33 to 77 days for the first donation to 66 to 114 days for the last donation. These donors reported symptoms of different intensity (from mild/moderate to severe), although none of them were hospitalized for COVID-19. Changes from baseline measurements were modeled with the use of a linear mixed-effects model for repeated measures based on a participant-level analysis with fixed effects for sex, age, and time since symptom onset (for more details, see supplemental Methods).
As shown in Figure 1A, the level of anti-RBD antibodies at the first donation varies greatly between donors. However, a decrease in anti-RBD antibody level between first and last donation was observed for all donors. To better illustrate the evolution of the anti-RBD antibody response over time, the relative level of anti-RDB antibodies was calculated at each time point using the first time point as reference (Figure 1B). In some donors, an increase was observed after their first donation, but this was always followed by a decline in anti-RBD antibodies at later time points. To rule out the possibility that the decline observed in all donors was a consequence of repeated donations, we determined the correlation between the number of donations and the overall decline in anti-RBD level, as defined using the maximal optical density (OD) and the OD at the last donation (ODlast donation/ODmax). As shown in Figure 1C, the decrease in anti-RBD levels did not correlate with the number of donations (r = .417, P = .1221). We then compared the decrease in anti-RBD level as a function of the time elapsed between the onset of symptoms and the time of the last donation (Figure 1D). The results revealed a significant correlation between these 2 parameters (r = .821, P = .0002), indicating that the anti-RBD response wanes over time of convalescence rather than because of repeated donations.
![Longitudinal analysis of the anti-RBD antibody response in 15 repeat CCP donors. Males and females with no history of pregnancy who recovered from a diagnosed COVID-19 infection were invited to donate plasma after informed consent. A volume of 500 to 750 mL plasma was collected by plasmapheresis (TRIMA Accel; Terumo BCT). Donors were allowed to donate plasma units every 6 days, for a maximum of 12 weeks. The level of anti-RBD antibodies was determined in our semiquantitative in-house ELISA (see supplemental Methods), using a 1:100 dilution of plasma. (A) Each curve represents the mean OD450nm ± SD obtained with the plasma of 1 donor at every donation (4-9 donations per donor) as a function of the days after symptom onset. The dotted line represents the cutoff value of the ELISA; some donors became seronegative at their last donation. (B) Same results but presented as the relative anti-RBD antibody level calculated at each time point using the first time point as reference: 1 − [OD450nm at each donation/OD450nm at first donation] × 100. (C) Correlation between the number of donations by each donor and the overall decline in anti-RBD level calculated using the following formula: 1 − [OD450nm at the last donation/maximal OD450nm obtained] × 100. (D) Correlation between the number of days between symptom onset and the last donation with the overall decline in anti-RBD level for each donor.](https://ash.silverchair-cdn.com/ash/content_public/journal/blood/136/22/10.1182_blood.2020008367/1/m_bloodbld2020008367f1.png?Expires=1769141979&Signature=ukWAmNJTcXofHXtCa6tvE~S98GFqGDXrM2Q0GYyldiEy2OH7Y2hATl5tfFFqmv~wiaBIAiEaEQusOvxxtjBLrMWt7~vxEUMv3Cml2l7q-mJFpZ8m5Th1sP940dhgfPJ8mEmYX-jUVqbf0Jyvv4tvyl07coeCWkp99n-dctgX3drT6AjvraXfyNM3VhewOhlNAfNnFF3UdWpkyFhT7TF3eoYx87C-3yESWwNHZ2bU~~JTBcD6xg8Yr22M20IvSDgcG3AkjwabkDbch84LqKhOEK0shsdZ17GLUJ~o1lA540LbsJfptzKzZA8I91dB~SbxHSIwyd9DgRLAu2r2wh1Mkg__&Key-Pair-Id=APKAIE5G5CRDK6RD3PGA)
Longitudinal analysis of the anti-RBD antibody response in 15 repeat CCP donors. Males and females with no history of pregnancy who recovered from a diagnosed COVID-19 infection were invited to donate plasma after informed consent. A volume of 500 to 750 mL plasma was collected by plasmapheresis (TRIMA Accel; Terumo BCT). Donors were allowed to donate plasma units every 6 days, for a maximum of 12 weeks. The level of anti-RBD antibodies was determined in our semiquantitative in-house ELISA (see supplemental Methods), using a 1:100 dilution of plasma. (A) Each curve represents the mean OD450nm ± SD obtained with the plasma of 1 donor at every donation (4-9 donations per donor) as a function of the days after symptom onset. The dotted line represents the cutoff value of the ELISA; some donors became seronegative at their last donation. (B) Same results but presented as the relative anti-RBD antibody level calculated at each time point using the first time point as reference: 1 − [OD450nm at each donation/OD450nm at first donation] × 100. (C) Correlation between the number of donations by each donor and the overall decline in anti-RBD level calculated using the following formula: 1 − [OD450nm at the last donation/maximal OD450nm obtained] × 100. (D) Correlation between the number of days between symptom onset and the last donation with the overall decline in anti-RBD level for each donor.
Longitudinal analysis of the anti-RBD antibody response in 15 repeat CCP donors. Males and females with no history of pregnancy who recovered from a diagnosed COVID-19 infection were invited to donate plasma after informed consent. A volume of 500 to 750 mL plasma was collected by plasmapheresis (TRIMA Accel; Terumo BCT). Donors were allowed to donate plasma units every 6 days, for a maximum of 12 weeks. The level of anti-RBD antibodies was determined in our semiquantitative in-house ELISA (see supplemental Methods), using a 1:100 dilution of plasma. (A) Each curve represents the mean OD450nm ± SD obtained with the plasma of 1 donor at every donation (4-9 donations per donor) as a function of the days after symptom onset. The dotted line represents the cutoff value of the ELISA; some donors became seronegative at their last donation. (B) Same results but presented as the relative anti-RBD antibody level calculated at each time point using the first time point as reference: 1 − [OD450nm at each donation/OD450nm at first donation] × 100. (C) Correlation between the number of donations by each donor and the overall decline in anti-RBD level calculated using the following formula: 1 − [OD450nm at the last donation/maximal OD450nm obtained] × 100. (D) Correlation between the number of days between symptom onset and the last donation with the overall decline in anti-RBD level for each donor.
To get a more general picture of the decline in anti-RBD antibodies over time, we performed a repeated-measure analysis with adjustment for donor age and sex. For group comparison, the time from onset of symptoms (33-114 days) was divided in quartiles containing similar numbers of samples (from 19 to 22 donor samples), and the data (OD values) in each of these quartiles were combined regardless of the donor identity. Figure 2 shows the distribution, median, and mean OD in each quartile. Overall, a significative decrease in OD value from baseline through last donation was observed (P < .0001). Pairwise comparisons showed that in the first and second quartiles (33-53 and 54-69 days after symptom onset, respectively), the median and mean OD were quite similar (mean, 1.499 ± 0.760 and 1.309 ± 0.710; median, 1.486 [interquartile range (IQR), 1.44] and 1.363 [IQR, 1.43], respectively, with P = .313), although a slight decrease in the mean values could be observed. This suggests that the anti-RBD response is relatively stable during the first 10 weeks after disease onset, in contrast with the recently reported decrease in neutralization activity in the plasma of convalescent patients a few weeks after symptom resolution.15,16,20-22 No significant decrease in median and mean OD values was observed between the second and third quartiles (54-69 and 70-84 days after symptom onset, respectively; mean, 1.309 ± 0.710 and 1.321 ± 0.720; median, 1.363 [IQR, 1.43] and 1.411 [IQR, 1.52], respectively, with P = .1205). However, the most striking observation comes from the comparison of the third and fourth quartiles (70-84 and 85-114 days after symptom onset, respectively), where a marked decrease in the mean OD values (significative mean OD decrease from 1.321 ± 0.720 to 0.835 ± 0.670, representing a 36.8% decrease with P = .0052) and an even more pronounced decrease in median values (median OD decreases from 1.411 [IQR, 1.52] to 0.411 [IQR, 1.15], representing a 70.1% decrease) were observed.
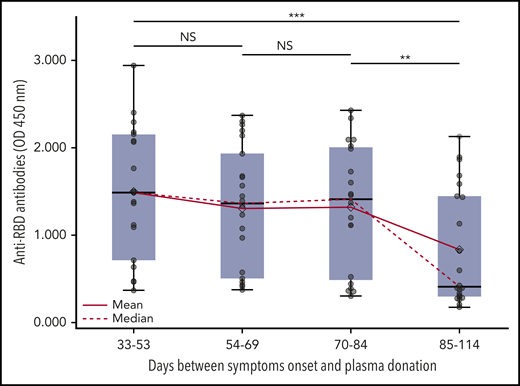
Evolution of the anti-RBD antibody response over time in repeat CCP donors. The time from onset of symptoms (33-114 days) was divided in quartiles containing similar numbers (between 19 and 22) of samples obtained from the donors shown in Figure 1. The mean and median OD450nm were calculated using all samples in each quartile. Each sample is represented by a dot. Boxes and horizontal bars denote IQR, whereas horizontal line and lozenge in boxes correspond to median and mean value, respectively. Whisker end points are equal to the maximum and minimum values below or above the median ± 1.5 times the IQR. Statistical significance was noted as not significant (NS). *P < .05; **P < .01; and ***P < .001.
Evolution of the anti-RBD antibody response over time in repeat CCP donors. The time from onset of symptoms (33-114 days) was divided in quartiles containing similar numbers (between 19 and 22) of samples obtained from the donors shown in Figure 1. The mean and median OD450nm were calculated using all samples in each quartile. Each sample is represented by a dot. Boxes and horizontal bars denote IQR, whereas horizontal line and lozenge in boxes correspond to median and mean value, respectively. Whisker end points are equal to the maximum and minimum values below or above the median ± 1.5 times the IQR. Statistical significance was noted as not significant (NS). *P < .05; **P < .01; and ***P < .001.
Interestingly, the decrease in OD values during a period of about 20 days (considering the mean and median of third and fourth quartiles, both of 76 and 95 days, respectively) is reminiscent of the plasma immunoglobulin G (IgG) half-life of 21 days,23 suggesting that de novo synthesis of anti-RBD antibodies stopped between the third and fourth quartiles in all CCP donors. This time frame is consistent with the first wave of a humoral immune response during which short-lived plasma cells actively secrete pathogen-specific antibodies until the antigen is eliminated.24 This is expected to be followed by the emergence of a cellular memory response that could play a major role in the long-term protection against reinfection, as recently proposed.25 The clinical significance of this in the event of re-exposure is therefore currently unknown.
Our study contains some limitations as only anti-RBD antibodies were measured in CCP from a limited number of different donors. Additional work including the characterization of our CCP donor plasma samples on other SARS-CoV-2 antigens (eg, full spike, nucleocapsid), the determination of the nAb titers, and contribution of antibody isotypes (IgA, IgG, and IgM) will permit extension of our initial observations on RBD antibodies to a broader humoral response to SARS-CoV-2 and help to better define its persistence. Nevertheless, the availability of sequential samples from the CCP repeated donors permitted to better pinpoint the time at which the anti-RBD response starts to significantly decline, regardless of the initial anti-RBD antibody level, which has been shown to correlate with disease severity.20,26,27 This observation has important implications for convalescent plasma collection especially because Xia et al28 recently provided data suggesting that the efficacy of CCP treatment in responder patients correlated with the antibody levels in CCP and for seroprevalence studies in the general population. Such studies should be performed close to the peak of infection, when most infected individuals (symptomatic or not) will still have easily detectable SARS-CoV-2 antibodies, to better estimate the true number of infections.
E-mail the corresponding author for original data.
The online version of this article contains a data supplement.
Acknowledgments
The authors are grateful to the convalescent plasma donors who participated in this study and the Héma-Québec team involved in convalescent donor recruitment and plasma collection. The authors also thank M. Gordon Joyce (US Military HIV Research Program) for the monoclonal antibody CR3022. All work was conducted in accordance with the Declaration of Helsinki in terms of informed consent and approval by an appropriate institutional board. Convalescent plasmas were obtained from donors who consented to participate in this research project at Héma-Québec (REB 2020-004).
This work was supported in part by Ministère de l’Économie et de l’Innovation du Québec, Programme de Soutien aux Organismes de Recherche et d’Innovation to A.F. A.F. is the recipient of Canada Research Chair on Retroviral Entry Grant RCHS0235 950-232424. G.B.-B. and J. Prévost are supported by Canadian Institutes of Health Research fellowships. P.B. is supported by a Fonds de Recherche du Québec-Santé Junior 2 Salary Award.
The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Authorship
Contribution: A.L., A.F., and R.B. conceived the study; J. Perreault, T.T., M.-J.F., M.D., G.B.-B., and J. Prévost performed and interpreted the experiments; A.L., P.B., A.F., and R.B. analyzed the data; A.L. and R.B. wrote the manuscript; and all authors read, edited, and approved the final manuscript.
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Correspondence: Renée Bazin, Héma-Québec, 1070 Ave des Sciences-de-la-Vie, Québec, QC G1V 5C3, Canada; e-mail: renee.bazin@hema-quebec.qc.ca.
