

In this issue of Blood, report an international, multicenter analysis of 198 patients with chronic lymphocytic leukemia (CLL) and symptomatic COVID-19.1 In this analysis, COVID-19 appears to be more severe in CLL patients than in the general population and, although risk factors are the same as for the general COVID-19 population, the outcome of patients needing admission is poor, with a case fatality rate of 37%. The Mato et al paper is particularly compelling as reports of COVID-19 in specific diseases are needed, particularly in cancer where COVID-19 adds to the physical and emotional distress these patients already suffer. Also, clinicians need guidance on how to advise and manage these patients.
CLL predominantly affects elderly people and is associated with immune dysfunction and, frequently, comorbidity; these factors overlap with those associated with severe COVID-19. Neither the prevalence of SARS-CoV-2 infection nor the distribution of clinical forms of COVID-19 in CLL patients is known. In the insert, the proportion of clinical forms of COVID-19 (mild, severe, critical) based on an analysis of 72 314 cases of COVID-19 in China is shown. Severe/critical cases account for 19% of patients. The case fatality rate observed in 2 studies analyzing the impact of COVID-19 in CLL patients is ∼37%.1,4
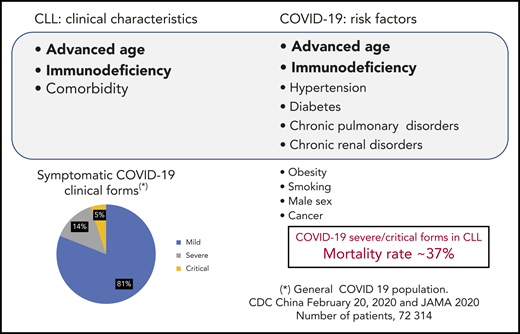
CLL predominantly affects elderly people and is associated with immune dysfunction and, frequently, comorbidity; these factors overlap with those associated with severe COVID-19. Neither the prevalence of SARS-CoV-2 infection nor the distribution of clinical forms of COVID-19 in CLL patients is known. In the insert, the proportion of clinical forms of COVID-19 (mild, severe, critical) based on an analysis of 72 314 cases of COVID-19 in China is shown. Severe/critical cases account for 19% of patients. The case fatality rate observed in 2 studies analyzing the impact of COVID-19 in CLL patients is ∼37%.1,4
Those with cancer are considered to be at a high risk for severe forms of COVID-19. Early reports indicated that ∼1% of patients with COVID-19 had cancer as an underlying condition.2 Cancer, older age, immunodeficiency, and many chronic diseases are widely recognized risk factors in COVID-19. CLL mainly affects the elderly (median age, 72 years) and is frequently associated with comorbidities and immunodeficiency. Also, infections (including viral and opportunistic) are the leading cause of death in this form of leukemia. Because of this, CLL patients are considered to have a high risk for infection with SARS-CoV-2 and for significant symptoms from COVID-19 disease (see figure). However, the prevalence of SARS-CoV-2 infection, risk factors for severe infection, the proportion of patients suffering from the different COVID-19 clinical forms (mild, severe, critical), and outcomes have not been established. Also, the optimal management and preventive measures remain to be determined.
A reasonable estimate of the prevalence of symptomatic COVID-19 in patients with CLL is ∼1%.2-4 The few studies published on COVID-19 in CLL have been limited to poor-risk subjects.1-4 Of note, although the proportion of cases with severe/critical COVID-19 in the general population is ∼20%,5 in CLL patients, it is unknown. In the Mato et al analysis, the case fatality rate of patients requiring admission was 37%, remarkably similar to that reported in a European cohort of 190 symptomatic patients (36.4%)4 . Not surprisingly, in this later study, the death rate was higher in the severe/critical group (91/151 or 60.3%) than in the mild group (15/39 or 38.5%) (P < .05).4 For reference, the mortality rate of 1591 persons (with only 81 or 8% with “malignancy”) admitted because of COVID-19 to intensive care units in Lombardia was 26%.6 In a general population with all forms of COVID-19 in China including 72 314 cases, the case fatality rate in patients with all types of cancer was 5.6% as compared with 2.3% in the general population.5 These data support the notion that some patients with CLL are at increased risk to develop severe/critical COVID-19. However, this should not be interpreted as the destiny of CLL patients is to contract severe, deadly COVID-19.
Besides the well-known, intertwined risk factors for COVID-19 (ie, age, chronic pulmonary disease, diabetes, chronic renal disorders, hypertension, obesity, smoking), are there other, disease-related factors for those with CLL? In the US study, age >75 years, Cumulative Illness Rating Scale >6, asthma, and chronic renal disorders predicted overall survival. In other words, the risk factors were mainly those known for COVID-19.,5 Hypogammaglobulinemia did not impact the outcome in either the US or the European cohorts.1,4 In the European survey, age >65 years correlated with the severity of the disease but not with mortality; comorbidity did not correlate with overall survival, either.4 These discrepancies may be due to methodological differences and selection bias (and illustrate the risks and weaknesses of indirect cross-comparisons of clinical studies).
In the Mato et al report, the overall survival of patients was not affected by CLL-directed therapy (mostly, ibrutinib), although in many cases therapy was withheld once COVID-19 was diagnosed. Conversely, in the European study, ibrutinib seemed to offer a protective effect.4 In some studies, the outcome of patients whose cancer was in remission at the time of COVID-19 diagnosis was significantly better than in those with uncontrolled cancer.7,8 Physicians should carefully balance the risks and benefits of CLL treatment, keeping in mind that active, uncontrolled CLL with severe COVID-19 is the worst possible scenario. In those patients requiring intervention, ibrutinib is now the best treatment option.9 An important caveat is that patients may die not because of COVID-19 but with COVID-19 (eg, superimposed infections, systemic complications), hence the importance of the best supportive medical care.
The role of immunity in COVID-19 is highly complex.10 In short, the accepted paradigm is that infection by SARS-CoV-2 (affecting primarily T lymphocytes, particularly CD4+ and CD8+ T cells) is followed by a rapid viral replication, unless it is controlled by an efficient immune system. If the virus is not controlled at this point, further viral replication may lead to cytokine-induced inflammatory storm, with severe pulmonary disease and disseminated thromboembolism. Patients with CLL do not have an efficient immune system. This results in a paradox: while a weakened immune system may not be capable of eliminating SARS-CoV-2, it might help to prevent a fatal immune and inflammatory overreaction. In fact, immunomodulators are being used and investigated in COVID-19. Also, there is interest in the potential role of ibrutinib as an immunomodulator. In CLL patients, Bruton tyrosine kinase (BTK) inhibitors could have a twofold benefit: controlling the leukemia and modulating the immune system. In the European cohort, ibrutinib did seem to exert a partial protective effect.4 In contrast, in the US study, treatment with ibrutinib did not protect from severe pulmonary disease.1 It is hoped that ongoing randomized trials will ascertain the role of ibrutinib (and other BTK inhibitors such as acalabrutinib) in the management of COVID-19. As dexamethasone has been reported to reduce death by up to one-third in patients with severe respiratory complications (www.recoverytrial.net), this agent should be given to those patients requiring ventilation, while it is further investigated. Hydroxychloroquine was not effective in the Mato et al study, confirming results from the RECOVERY trial (www.recoverytrial.net).
Addressing the impact of COVID-19 on specific diseases is a medical necessity. These studies are particularly urgent in hematologic malignancies due to their intrinsic and treatment-related immune defects that may increase the risk for COVID-19. Well-designed prospective studies based on large series of patients are needed. Effective therapies for COVID-19 and vaccines are eagerly awaited. Meanwhile, and as long as the COVID-19 outbreak persists, patients with CLL should maintain standard preventive measures (ie, hand washing, safe interpersonal distance, masks) and be managed, whenever possible, in CLL reference centers with COVID-19–free facilities and telemedicine resources.
Conflict-of-interest disclosure: The author declares no competing financial interests.
