

A 37-year-old man presented to our clinic with persistent fatigue and dyspnea on exertion after receiving cladribine treatment 6 months earlier for hairy cell leukemia (HCL), diagnosed in another hospital. Complete blood count was normal, and splenomegaly was absent. Bone marrow (BM) examination, to reassess disease status, revealed a population of large-sized lymphocytes, with abundant cytoplasm and oval nuclei (panel A, black arrows), with an unexpected intrasinusoidal pattern of infiltration, positive for CD20 (panel B), CD103 (panel C), DBA44/CD72, CD25, CD11c, Cyclin-D1, and Annexina-A1 at immunohistochemical essay, accounting for ∼15% of BM cellularity. Reticulin fibrosis was grade 1. Immunostaining for mutated BRAF protein (panel D) confirmed the diagnosis of HCL persistence; BRAF V600E mutation was detected on BM blood sample.
BM involvement by HCL usually consists of interstitial or “patchy” infiltrates made of widely spaced mononuclear cells. Erythrocytes are frequently seen in infiltrated areas, extravasated, or surrounded by neoplastic cells. Intrasinusoidal pattern of infiltration is exceptionally rare in HCL, whereas it is typically described in lymphomas such as splenic marginal zone lymphoma, splenic diffuse red pulp small B–cell lymphoma, and HCL variant. These malignancies may share common clinical and immunophenotypic hallmarks with HCL; therefore, the identification of V600E BRAF mutation is mandatory to render a correct diagnosis.
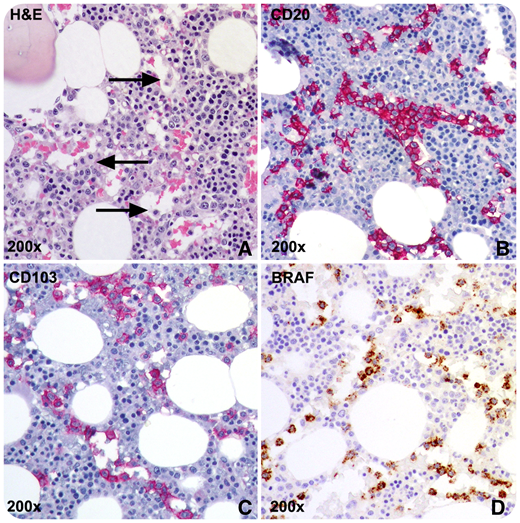
A 37-year-old man presented to our clinic with persistent fatigue and dyspnea on exertion after receiving cladribine treatment 6 months earlier for hairy cell leukemia (HCL), diagnosed in another hospital. Complete blood count was normal, and splenomegaly was absent. Bone marrow (BM) examination, to reassess disease status, revealed a population of large-sized lymphocytes, with abundant cytoplasm and oval nuclei (panel A, black arrows), with an unexpected intrasinusoidal pattern of infiltration, positive for CD20 (panel B), CD103 (panel C), DBA44/CD72, CD25, CD11c, Cyclin-D1, and Annexina-A1 at immunohistochemical essay, accounting for ∼15% of BM cellularity. Reticulin fibrosis was grade 1. Immunostaining for mutated BRAF protein (panel D) confirmed the diagnosis of HCL persistence; BRAF V600E mutation was detected on BM blood sample.
BM involvement by HCL usually consists of interstitial or “patchy” infiltrates made of widely spaced mononuclear cells. Erythrocytes are frequently seen in infiltrated areas, extravasated, or surrounded by neoplastic cells. Intrasinusoidal pattern of infiltration is exceptionally rare in HCL, whereas it is typically described in lymphomas such as splenic marginal zone lymphoma, splenic diffuse red pulp small B–cell lymphoma, and HCL variant. These malignancies may share common clinical and immunophenotypic hallmarks with HCL; therefore, the identification of V600E BRAF mutation is mandatory to render a correct diagnosis.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal