

The patient is a 66-year-old Middle Eastern woman who presented with B symptoms (severe fatigue, night sweats, and fever), weight loss, anemia, and splenomegaly with elevated liver enzymes and respiratory insufficiency. Bone marrow biopsy showed a B-lymphocyte population with pleomorphic nuclei and prominent nucleoli that expanded the bone marrow sinusoids (panel A, hematoxylin and eosin stain, 40× objective, original magnification ×400) and was highlighted by PAX5 (panel C, PAX5 immunohistochemical study, 20× objective, original magnification ×200) and CD20 (panel D, CD20 immunohistochemical study, 20× objective, original magnification ×200). Hemophagocytosis was present (panel B, Wright-Giemsa stain, 60× objective, original magnification ×600). Immunohistochemical studies showed the lymphoma cells to be positive for CD20, PAX5, CD5, BCL2, BCL6 (dim), MUM1, and LEF1 and negative for CD10, SOX11, c-MYC, and PD-L1. No other tissue biopsy was performed.
Intravascular large B-cell lymphoma is a rare aggressive lymphoma that shows growth within small vessels often with widespread dissemination. Three clinically distinct variants have been identified: classical variant (with frequent central nervous system, cutaneous, and endocrine involvement), cutaneous variant (with involvement limited to the skin), and hemophagocytic syndrome (HPS)-associated variant (with a typical HPS presentation). Previously, the HPS-associated variant was described as the Asian variant due to its near-exclusive presentation in patients of Asian ancestry, as in this case. Despite the different extent of involvement between the classical and HPS-associated variants, prognosis in both is extremely poor with this aggressive lymphoma. Recent studies have shown frequent mutations in CD79B and MYD88, which may present future avenues for targeted therapy.
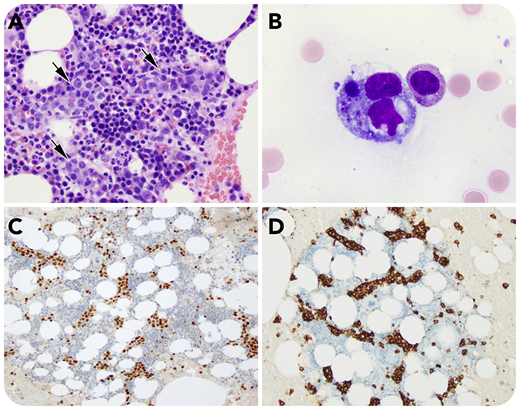
The patient is a 66-year-old Middle Eastern woman who presented with B symptoms (severe fatigue, night sweats, and fever), weight loss, anemia, and splenomegaly with elevated liver enzymes and respiratory insufficiency. Bone marrow biopsy showed a B-lymphocyte population with pleomorphic nuclei and prominent nucleoli that expanded the bone marrow sinusoids (panel A, hematoxylin and eosin stain, 40× objective, original magnification ×400) and was highlighted by PAX5 (panel C, PAX5 immunohistochemical study, 20× objective, original magnification ×200) and CD20 (panel D, CD20 immunohistochemical study, 20× objective, original magnification ×200). Hemophagocytosis was present (panel B, Wright-Giemsa stain, 60× objective, original magnification ×600). Immunohistochemical studies showed the lymphoma cells to be positive for CD20, PAX5, CD5, BCL2, BCL6 (dim), MUM1, and LEF1 and negative for CD10, SOX11, c-MYC, and PD-L1. No other tissue biopsy was performed.
Intravascular large B-cell lymphoma is a rare aggressive lymphoma that shows growth within small vessels often with widespread dissemination. Three clinically distinct variants have been identified: classical variant (with frequent central nervous system, cutaneous, and endocrine involvement), cutaneous variant (with involvement limited to the skin), and hemophagocytic syndrome (HPS)-associated variant (with a typical HPS presentation). Previously, the HPS-associated variant was described as the Asian variant due to its near-exclusive presentation in patients of Asian ancestry, as in this case. Despite the different extent of involvement between the classical and HPS-associated variants, prognosis in both is extremely poor with this aggressive lymphoma. Recent studies have shown frequent mutations in CD79B and MYD88, which may present future avenues for targeted therapy.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal