

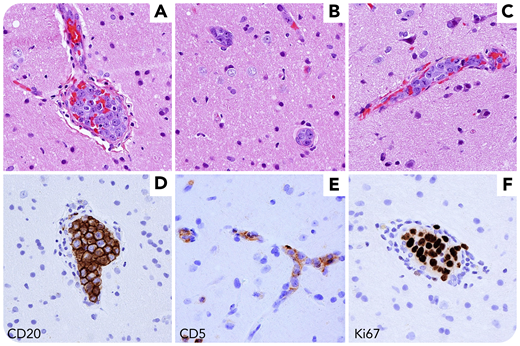
A 58-year-old man presented acutely delirious and confused, initially presumed secondary to alcohol withdrawal. Subsequently, computed tomography imaging showed bilateral areas of encephalomalacia. Brain biopsy revealed preserved brain parenchyma with large mitotically active atypical lymphoid cells occupying numerous blood vessels and capillaries (panels A-C, hematoxylin and eosin, original magnification ×400). Atypical cells outside of the vessels were not seen. The large blastic cells expressed CD20 and CD5 and were highly proliferative by Ki67 staining (panels D-F, original magnification ×400). Additional stains demonstrated non–germinal center immunophenotype and overexpression of MYC and BCL2. The patient was diagnosed with intravascular large B-cell lymphoma (IVLBCL), a lymphoma with exclusively intravascular growth and variable large cell morphology.
IVLBCL is a rare lymphoma, usually diagnostically challenging owing to its rarity and variable clinical presentation. Symptomatology, often including skin changes, neurologic dysfunction, and B symptoms, depends on the pattern of organ involvement, which can be any (excluding lymph nodes). Histologic findings are characteristic, with large atypical lymphoid cells filling capillaries and small- to medium-sized blood vessels. Non–germinal center immunophenotype is typical, often with CD5 positivity. Dual BCL2/MYC overexpression has been reported, but its significance is unclear. The clinical course is generally very aggressive, except for skin-limited disease. Treatment relies on multiagent chemotherapy with rituximab.
A 58-year-old man presented acutely delirious and confused, initially presumed secondary to alcohol withdrawal. Subsequently, computed tomography imaging showed bilateral areas of encephalomalacia. Brain biopsy revealed preserved brain parenchyma with large mitotically active atypical lymphoid cells occupying numerous blood vessels and capillaries (panels A-C, hematoxylin and eosin, original magnification ×400). Atypical cells outside of the vessels were not seen. The large blastic cells expressed CD20 and CD5 and were highly proliferative by Ki67 staining (panels D-F, original magnification ×400). Additional stains demonstrated non–germinal center immunophenotype and overexpression of MYC and BCL2. The patient was diagnosed with intravascular large B-cell lymphoma (IVLBCL), a lymphoma with exclusively intravascular growth and variable large cell morphology.
IVLBCL is a rare lymphoma, usually diagnostically challenging owing to its rarity and variable clinical presentation. Symptomatology, often including skin changes, neurologic dysfunction, and B symptoms, depends on the pattern of organ involvement, which can be any (excluding lymph nodes). Histologic findings are characteristic, with large atypical lymphoid cells filling capillaries and small- to medium-sized blood vessels. Non–germinal center immunophenotype is typical, often with CD5 positivity. Dual BCL2/MYC overexpression has been reported, but its significance is unclear. The clinical course is generally very aggressive, except for skin-limited disease. Treatment relies on multiagent chemotherapy with rituximab.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal