

A 72-year-old woman presented with a 2-year history of splenomegaly, thrombocytopenia, and transfusion-dependent Coombs-negative hemolytic anemia. She visited Long Island for the past 2 summers. After her most recent trip, she experienced intermittent fevers and chills with no identifiable etiologies. After splenectomy to evaluate for occult lymphoproliferative disorder, her symptoms resolved, but recurred 3 weeks later. Upon admission, she met the criteria for hemophagocytic lymphohistiocytosis (HLH) based on ferritin (15 174 ng/mL), triglyceride (291 mg/dL), soluble interleukin 2 receptor (41 500 pg/mL), fibrinogen (132 mg/dL), hemoglobin (7.5 g/dL), and platelet (41 000/µL) parameters. The spleen showed histiocytes phagocytosing erythrocytes (panel A, black arrows) and nucleated cells (panel A, open arrows; original magnification ×600, ×60 objective, hematoxylin and eosin stain). She was started on etoposide and dexamethasone for HLH. Because of persistent pancytopenia and fevers, peripheral blood smears were evaluated, revealing numerous intracellular ring forms (panel B), tetrad-forms or “Maltese Cross” (panel C), and extracellular protozoa in isolation (panel D) or clusters (panel E; panels B-E: original magnification ×1000, ×100 objective, Wright stain). Positive Babesia microti immunoglobulin M and immunoglobulin G antibody titers confirmed babesiosis. After 4 weeks of HLH induction regimen, azithromycin and atovaquone, and a single exchange transfusion, her symptoms, HLH parameters, and parasitemia improved markedly.
In the United States, babesiosis is transmitted via Ixodes scapularis or blood transfusion, can cause secondary HLH, and may require serial blood smear examinations for diagnosis.
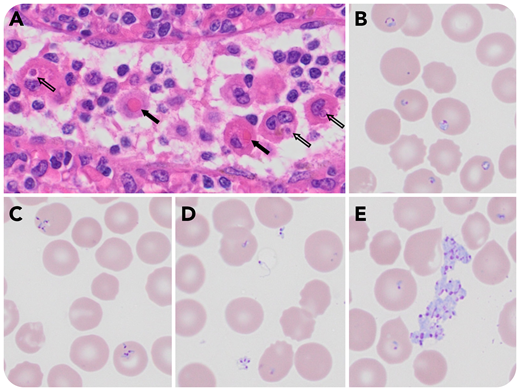
A 72-year-old woman presented with a 2-year history of splenomegaly, thrombocytopenia, and transfusion-dependent Coombs-negative hemolytic anemia. She visited Long Island for the past 2 summers. After her most recent trip, she experienced intermittent fevers and chills with no identifiable etiologies. After splenectomy to evaluate for occult lymphoproliferative disorder, her symptoms resolved, but recurred 3 weeks later. Upon admission, she met the criteria for hemophagocytic lymphohistiocytosis (HLH) based on ferritin (15 174 ng/mL), triglyceride (291 mg/dL), soluble interleukin 2 receptor (41 500 pg/mL), fibrinogen (132 mg/dL), hemoglobin (7.5 g/dL), and platelet (41 000/µL) parameters. The spleen showed histiocytes phagocytosing erythrocytes (panel A, black arrows) and nucleated cells (panel A, open arrows; original magnification ×600, ×60 objective, hematoxylin and eosin stain). She was started on etoposide and dexamethasone for HLH. Because of persistent pancytopenia and fevers, peripheral blood smears were evaluated, revealing numerous intracellular ring forms (panel B), tetrad-forms or “Maltese Cross” (panel C), and extracellular protozoa in isolation (panel D) or clusters (panel E; panels B-E: original magnification ×1000, ×100 objective, Wright stain). Positive Babesia microti immunoglobulin M and immunoglobulin G antibody titers confirmed babesiosis. After 4 weeks of HLH induction regimen, azithromycin and atovaquone, and a single exchange transfusion, her symptoms, HLH parameters, and parasitemia improved markedly.
In the United States, babesiosis is transmitted via Ixodes scapularis or blood transfusion, can cause secondary HLH, and may require serial blood smear examinations for diagnosis.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal