

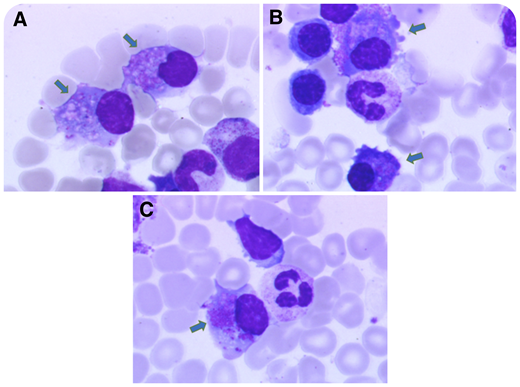
A 60-year-old man with a 1-year history of chronic kidney disease (estimated glomerular filtration rate 53 mL/min per 1.73 m2) and hypouricemia was referred for nephrology work-up. He had hypophosphatemia, proteinuria (0.94 mg/mg), and normoglycemic glycosuria. Kidney biopsy was consistent with Fanconi syndrome (FS), and serum immunofixation showed monoclonal κ light chains (LCs). The bone marrow (BM) smear showed 6% plasma cells (PCs) (see panels A-C for 3 aspects), with crystalline cytoplasmic inclusions (see arrows, original magnification ×1000; May-Grünwald Giemsa stain) and abnormal phenotype by flow cytometry (CD19lo, CD117+, monotypic κ). Targeted next-generation sequencing (NGS) showed partial 11q gain, translocation t(11;14), and clonal IRF4 mutation.
FS is a rare disorder of renal proximal tubule (PT) transport that is characterized by type 2 acidosis with urinary leak of phosphate, uric acid, glucose, and amino acids. Most adult cases are acquired and drug related, but FS can be associated with monoclonal gammopathies. The monoclonal component is usually mild with κ LC restriction (Vκ1 subgroup of variability) with CDR1 mutations. This leads to unusual hydrophobic residues, resistance to proteolysis, and injuries in the PT. Toxic κ LCs form crystals within the endolysosomal compartment of PT cells and BM PCs. In this case, NGS revealed t(11:14) that is frequent in LC diseases and clonal IRF4 mutation that could enhance V(D)J rearrangement at the κ locus.
A 60-year-old man with a 1-year history of chronic kidney disease (estimated glomerular filtration rate 53 mL/min per 1.73 m2) and hypouricemia was referred for nephrology work-up. He had hypophosphatemia, proteinuria (0.94 mg/mg), and normoglycemic glycosuria. Kidney biopsy was consistent with Fanconi syndrome (FS), and serum immunofixation showed monoclonal κ light chains (LCs). The bone marrow (BM) smear showed 6% plasma cells (PCs) (see panels A-C for 3 aspects), with crystalline cytoplasmic inclusions (see arrows, original magnification ×1000; May-Grünwald Giemsa stain) and abnormal phenotype by flow cytometry (CD19lo, CD117+, monotypic κ). Targeted next-generation sequencing (NGS) showed partial 11q gain, translocation t(11;14), and clonal IRF4 mutation.
FS is a rare disorder of renal proximal tubule (PT) transport that is characterized by type 2 acidosis with urinary leak of phosphate, uric acid, glucose, and amino acids. Most adult cases are acquired and drug related, but FS can be associated with monoclonal gammopathies. The monoclonal component is usually mild with κ LC restriction (Vκ1 subgroup of variability) with CDR1 mutations. This leads to unusual hydrophobic residues, resistance to proteolysis, and injuries in the PT. Toxic κ LCs form crystals within the endolysosomal compartment of PT cells and BM PCs. In this case, NGS revealed t(11:14) that is frequent in LC diseases and clonal IRF4 mutation that could enhance V(D)J rearrangement at the κ locus.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal