

Background: The CD38-targeting antibody daratumumab, when combined with a proteasome inhibitor or with an immunomodulatory agent (IMiD) increases depth and duration of response in multiple myeloma (MM). Depth of remission post initial therapy as assessed by MRD predicts long term outcome in NDMM. We hypothesized that the combination of daratumumab, carfilzomib, lenalidomide and dexamethasone (Dara-KRd) would be safe and highly active in patients with NDMM. In addition, we assessed the feasibility of using MRD by next generation sequencing (clonoSEQ® method, sensitivity 10-6) to inform the use and duration of post-transplant Dara-KRd consolidation.
Methods: Eligible patients (pts) had NDMM requiring treatment, creatinine clearance >40 ml/min, adequate liver and cardiac function, ECOG performance status 0-2 with no age limit. Treatment cycles consisted of daratumumab 16 mg/kg IV days 1,8,15,22 (with typical reduction in frequency with subsequent cycles), carfilzomib 56 mg/m2 IV days 1,8,15, lenalidomide 25 mg PO days 1-21 and dexamethasone 40 mg PO/IV days 1,8,15,22 repeated every 28 days. Patients received 4 cycles of Dara-KRd as induction, autologous transplantation, and received 0, 4 or 8 cycles of Dara-KRd consolidation, according to MRD status at each phase of therapy. MRD was evaluated by clonoSEQ® (NGS-MRD; Adaptive Biotechnologies, Seattle, WA) at end of induction, post-transplant, and during each 4-cycle block of Dara-KRd consolidation. Primary endpoint was achievement of MRD negative remission (<10-5) as defined by IMWG consensus. Secondary endpoints included MRD <10-6, complete response (CR) by IMWG criteria at end of induction and upon completion of consolidation, and rate of imaging (assessed by PET/CT scan) plus MRD-negative CR. Patients received therapy until achievement of two consecutive MRD reads <10-5 (confirmed MRD-negative remission; e.g., post-induction and post-transplant or post-transplant and during consolidation). Confirmed MRD-negative pts received no further therapy and were observed with surveillance for MRD resurgence 6 and 18 months after treatment discontinuation. Patients completing consolidation without confirmed MRD-negative remission received standard lenalidomide maintenance (NCT03224507).
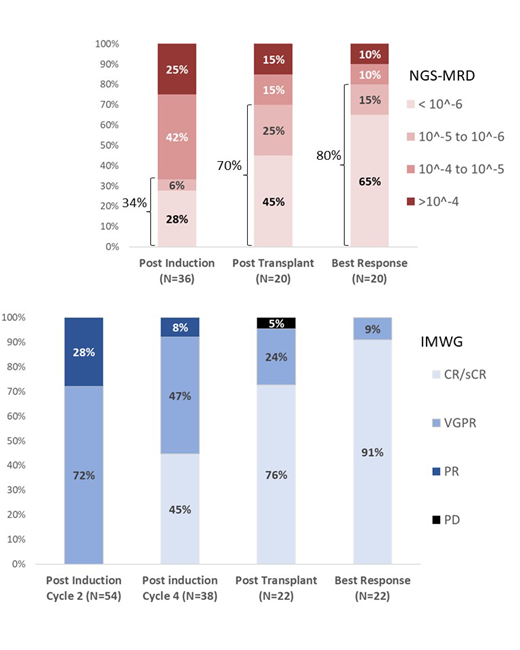
Results: Currently 69 pts have been enrolled, 38 have completed induction and 22 have completed post-transplant assessment. Median age was 61 (range 38-79) years, 13 (19%) had ISS 3, and 20 (29%) had high-risk chromosomal abnormalities [del17p, t(4;14) or t(14;16)]. Sixty-six (96%) pts had MRD trackable by clonoSEQ® and 100% of the expected MRD datapoints were successfully obtained. All patients responded by end of induction cycle 2, 92% of pts obtained VGPR or better after induction and 91% of patients who have reached transplant obtained CR/sCR as best response on therapy (Figure). MRD-negative remission (<10-5) rate was 34%, 70% and 80% after induction, transplant and at best response, respectively (Figure). Rates of MRD <10-6 were 28%, 45% and 65% respectively. No patient discontinued therapy due to toxicity. One patient died from metapneumovirus pneumonia post-transplant, considered not related to investigational agents. Most common grade 3 and 4 AEs were neutropenia (n=7), infection (n=6), insomnia (n=4), hyperglycemia (n=2) and rash (n=2). There were 15 serious AEs including pneumonia (n=5), fever and neutropenia (n=2), pulmonary embolism (n=1), and atypical hemolytic uremic syndrome (n=1). All 11 patients who have achieved confirmed MRD-negative remission and discontinued therapy also achieved imaging plus MRD-negative CR and none had relapse or resurgence of MRD with short follow up (0.8-7.3 months). Longer follow-up, post-induction and post-transplant MRD assessment for at least 69 and 41 pts, respectively, will be presented at the meeting.
Conclusion: This is the first report of monoclonal antibody-based quadruplet regimen with MRD-based response-adapted therapy in NDMM. Dara-KRd induction, autologous transplant and Dara-KRd consolidation guided by MRD is feasible, safe and leads to high proportion of patients achieving CR/sCR, IMWG MRD-negative CR, imaging plus MRD-negative CR and MRD <10-6. This approach can form the basis for clinical efforts to reduce the burden of continuous therapy in those with confirmed MRD-negative remissions.
Costa:Amgen: Consultancy, Honoraria, Research Funding, Speakers Bureau; Janssen: Research Funding, Speakers Bureau; Celgene: Consultancy, Honoraria, Research Funding; Sanofi: Consultancy, Honoraria, Speakers Bureau; GSK: Consultancy, Honoraria, Research Funding; Abbvie: Consultancy; Karyopharm: Consultancy; Fujimoto Pharmaceutical Corporation Japan: Other: Advisor. Cornell:Takeda: Consultancy; KaryoPharm: Consultancy. Silbermann:Janssen, Sanofi: Other: Consultant/Advisor. Dhakal:Amgen: Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene: Honoraria; Takeda: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees; Sanofi: Membership on an entity's Board of Directors or advisory committees. Omel:Celgene, Takeda, Janssen: Other: Patient Advisory Committees. Hari:Kite: Consultancy, Honoraria; Janssen: Consultancy, Honoraria; BMS: Consultancy, Research Funding; AbbVie: Consultancy, Honoraria; Cell Vault: Equity Ownership; Sanofi: Honoraria, Research Funding; Spectrum: Consultancy, Research Funding; Amgen: Research Funding; Celgene: Consultancy, Honoraria, Research Funding; Takeda: Consultancy, Honoraria, Research Funding.
Carfilzomib for newly diagnosed multiple myeloma

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal