

Background: Despite recent advances in the therapeutic armamentarium for AML, outcomes remain dismal for patients (pts) with relapsed/refractory (R/R) AML. Response rates with high dose cytarabine (HiDAC) salvage chemotherapy are approximately 20%. Multiple immune aberrations in AML lead to immune suppression, exhaustion, and senescence. Programmed Death-1 (PD-1), a co-inhibitory receptor (IR) on immune cells, suppresses immune activation and is exploited by leukemic cells to evade immune surveillance. PD-1 and other IRs are up-regulated during disease progression. We hypothesized that pembrolizumab, a monoclonal antibody targeting PD-1, after HiDAC would stimulate a T-cell mediated anti-leukemic immune response.
Methods: Eligibility for this study included R/R AML 18-70 years, ECOG PS 0-1 and adequate organ function. Treatment consisted of HiDAC (<60 years: 2 gm/m2 IV Q12hours days 1-5; >60 years: 1.5 gm/m2 IV Q12hours days 1-5) followed by pembrolizumab 200 mg IV on day 14. The primary objective of this study was to estimate the overall complete remission (CR + CRi) rate. Secondary objectives included assessment of safety, durability of CR, overall survival (OS) and biomarker correlates of response. Overall responders were eligible to receive maintenance phase pembrolizumab 200 mg IV Q3weeks for up to 2 years until progression. Allogeneic stem cell transplant (alloSCT) was permissible before or after maintenance phase.
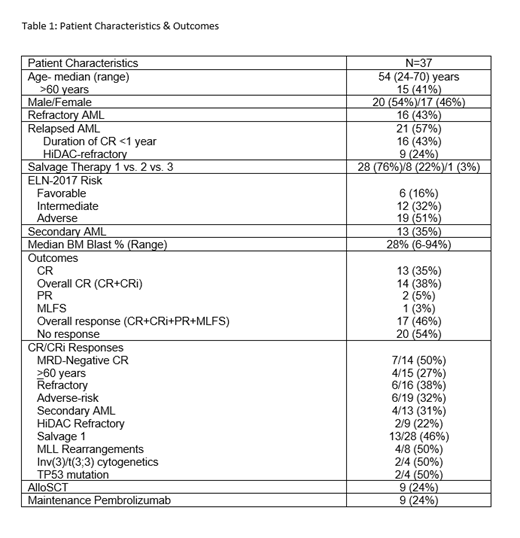
Results: Thirty-seven pts were enrolled and evaluable (Table 1). Sixteen (43%) pts had refractory disease and 16 (43%) pts had relapsed AML with CR1 duration <1 year. Excluding electrolyte abnormalities, the most common pembrolizumab-related toxicities were febrile neutropenia (57%), ALT elevation (43%; Grade >3: n=1), AST elevation (32%; Grade >3: n=1), fatigue (27%), alkaline phosphatase elevation (24%), and maculopapular rash (19%; Grade >3: n=2). Grade >3 immune-related adverse events (iRAE) were rare (maculopapular rash: n=2, AST/ALT increase: n=2, right upper quadrant pain with lymphocytic infiltrate in liver: n=1) and self-limiting. Five (14%) pts required steroid administration for grade 2 hyperbilirubinemia (n=1), grade 3 ALT elevation (n=1), grade 3 AST elevation with liver biopsy revealing no evidence of iRAE (n=1), grade 3 bilirubin subsequently deemed to be a delayed hemolytic transfusion reaction (n=1), and grade 3 systolic dysfunction without evidence of myocarditis by endomyocardial biopsy or cardiac MRI (n=1). Sixty-day mortality was 3% (1/37) due to progressive AML. Median time to full neutrophil (>1x109/L) and platelet (>100x109/L) recovery was 32 and 31 days, respectively.
The overall response (ORR: CR+CRi+PR+MLFS) and composite CR (CR+CRi) rates were 46% [29%,63%] and 38% [22%,55%], respectively, meeting the primary endpoint of the study. Notably, 13/28 (46%) pts receiving HiDAC + pembrolizumab as their first salvage regimen achieved CR/CRi. Two pts refractory to HiDAC (administered within past 6 months) achieved CR including one pt who was refractory to HiDAC salvage 1 month prior to enrollment and ultimately achieved CR without evidence of minimal residual disease. Nine (24%) pts received an alloSCT. There were no instances of Grade >3 acute GVHD or veno-occlusive disease post-alloSCT. Nine (24%) pts received maintenance phase pembrolizumab (median # of cycles = 3; range: 1-12) for CR (n=8) or PR (n=1). Seven out of 9 pts relapsed/progressed after maintenance phase. Median follow-up among survivors, and median OS, event-free survival and disease-free survival was 7.8 months, 8.9 months [6.0,13.1], 6.9 months [4.2,11.5], and 5.7 months [1.9,7.3], respectively.
Conclusions: Pembrolizumab can be safely administered after HiDAC salvage in R/R AML. Severe iRAE's were uncommon despite administration after cytotoxic chemotherapy. The addition of pembrolizumab to HiDAC led to an encouraging overall CR rate meeting the primary endpoint of the study. Immunogenomic biomarker analyses consisting of B cell receptor amplicon sequencing, RNA-seq of blasts and CD8+ T cells, CD8+ T cell receptor repertoire, whole exome sequencing and flow cytometry analyses are ongoing to determine predictors of response. These results warrant further investigation of IR blockade and other immunomodulatory therapeutic strategies after intensive cytotoxic chemotherapy in AML.
Zeidner:Takeda: Research Funding; Merck: Research Funding; AsystBio Laboratories: Consultancy; Pfizer: Honoraria; Tolero: Honoraria, Research Funding; Daiichi Sankyo: Honoraria; Celgene: Consultancy, Honoraria, Research Funding; Agios: Honoraria; AbbVie: Honoraria. Vincent:Pharmacyclics: Research Funding; Merck: Research Funding. Foster:Bellicum Pharmaceuticals: Research Funding; Macrogenics: Research Funding; Celgene: Research Funding; Daiichi Sankyo: Consultancy. Coombs:Dedham Group: Consultancy; Covance: Consultancy; Cowen & Co.: Consultancy; Octopharma: Honoraria; H3 Biomedicine: Honoraria; Loxo: Honoraria; Pharmacyclics: Honoraria; Medscape: Honoraria. Webster:Pfizer: Consultancy; Amgen: Consultancy; Genentech: Research Funding. DeZern:Astex Pharmaceuticals, Inc.: Consultancy; Celgene: Consultancy. Smith:Jazz: Consultancy; Pfizer: Consultancy; Novartis: Consultancy; Agios: Consultancy. Levis:Amgen: Consultancy, Honoraria; Astellas: Consultancy, Research Funding; FUJIFILM: Consultancy, Research Funding; Menarini: Consultancy, Honoraria; Novartis: Consultancy, Research Funding; Daiichi Sankyo Inc: Consultancy, Honoraria; Agios: Consultancy, Honoraria. Luznik:Merck: Research Funding, Speakers Bureau; Genentech: Research Funding; AbbVie: Consultancy; WindMiL Therapeutics: Patents & Royalties: Patent holder. Serody:Merck: Research Funding; GlaxoSmithKline: Research Funding. Gojo:Amphivena: Research Funding; Amgen Inc: Consultancy, Honoraria, Research Funding; Juno: Research Funding; Merck: Research Funding; Jazz: Consultancy, Honoraria; Novartis: Consultancy, Honoraria; Abbvie: Consultancy, Honoraria.
Pembrolizumab is investigational for AML.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal