

Background: Early progression of disease (POD) in patients (pts) with mantle cell lymphoma (MCL) following intensive frontline treatment has been associated with inferior survival (Dietrich et al Ann Oncol 2014 and Visco et al Br J Haematol 2019), but the optimal time point to define early POD and the predictive significance of early POD following less intensive frontline treatment is not well established. We compare outcomes after all frontline treatments in a large MCL cohort categorized by time to progression and describe outcomes by class of second line treatment for pts with primary refractory disease.
Methods: Clinical and outcome data for MCL pts treated between 2000 and 2017 were collected from 12 US centers. Overall survival (OS), defined from time of 1st progression, and secondary progression free survival (PFS2), defined from 1st progression to 2nd progression or death, were estimated by Kaplan-Meier and compared by log-rank test. Univariable and multivariable analyses were performed using Cox proportional hazards models for OS. 95% confidence intervals were calculated for all estimates and displayed in square brackets.
We defined intensive treatment as high dose cytarabine in frontline therapy and/or autologous stem cell transplant in 1st remission. Pts were categorized into three groups: (a) refractory disease to frontline therapy or POD within 6 months of frontline therapy was termed primary refractory (PRF); (b) POD between 6 to 24 months of therapy was termed POD24 and (c) POD beyond 24 months was termed POD>24. Salvage therapy was categorized as chemoimmunotherapy (CIT) for pts treated with CIT alone, BTK inhibitor (BTKi) for pts treated with BTKi single agent or in combination, and lenalidomide / bortezomib for pts treated with one or both agent +/- anti-CD20 therapy.
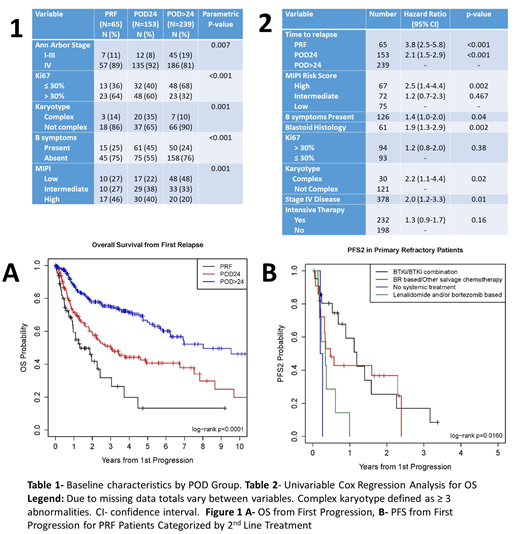
Results: Of 1,168 pts with MCL, 457 pts had relapsed and were included in this analysis. The median age was 62, 77% were male, and ECOG PS was 0/1 in 94%. Median follow-up was 2.6 years (yr) after first progression. The most common induction regimens were R-HyperCVAD (26%), R-CHOP (24%), bendamustine and rituximab (19%), and R-M-CHOP (10%). Frontline treatment was intensive in 54%. Sixty five pts (14%) were PRF, 153 (34%) had POD24, and 239 (53%) had POD>24. Additional baseline characteristics and comparison between groups are summarized in Table 1.
The median OS was 1.3 yr [0.9-2.4] for PRF pts, 3 yrs [2-6.8] for POD 24, and 8 yrs [6.2-not reached (NR)] for POD>24 (p<0.0001). Comparing median PFS2 by time to POD, median PFS2 was 1 yr [0.4-1.3] for PRF, 1 yr [0.8-1.4] for POD24 and 2.3 yrs [1.8-3.2] for POD>24 pts (p<0.0001). Among PRF pts, median OS was 0.9 yr [0.4-3] for intensive treatment pts versus 2.0 yrs [0.9-4.5] among less intensive treatment (p=0.33). Among POD24 pts, median PFS2 was 0.8 yr [0.5-1] following intensive vs 2 yrs [0.8-2.9] with less intensive treatment (p=0.0003); likewise OS was shorter after intensive vs less intensive treatment, median 2 yrs [1.1-3.4] vs 6.8 yrs [3.1-9.7] (p=0.05). Both PRF and POD24 were associated with inferior OS on univariable analysis (Table 2) and remained associated with inferior OS on multivariable analysis independent of MIPI score and B symptoms (sx); HR 7.7 [3.9-15.1] for PRF and HR 2.5 [1.4-4.5] for POD24, HR 2.5 [1.4-4.5] for high MIPI score, and HR 1.3 [0.8-2.2] for B sx.
Among pts with PRF MCL, median PFS2 and OS were 1.2 [0.5-2.3] and 2.4 [0.7-4.5] yrs for BTKi (n=21), 0.5 [0.2-2.3] and 1.1 [0.5-NR] yrs for CIT (n=22), and 0.3 [0.1-0.6] and 1.9 [0.1-2] yrs for lenalidomide / bortezomib (n=8) as 2nd line therapy. Two pts with PRF MCL received no further therapy and both died within one month of POD.
Conclusions: Time to relapse is predictive of outcome in pts with MCL and outcomes with current salvage therapies are poor for pts with relapse within 6 months of frontline therapy. Of currently available second line therapies, BTKi were associated with improved PFS2 in refractory pts. Outcomes are particularly poor for pts who receive intensive induction therapies yet still relapse early, representing a population at high risk for early mortality related to MCL. Novel treatment approaches should be evaluated in this population, including CAR-T cell therapy, and attempts to improve risk stratification at diagnosis and develop improved therapies for high-risk pts should continue.
Maddocks:Pharmacyclics: Membership on an entity's Board of Directors or advisory committees, Research Funding; BMS: Research Funding; Merck: Research Funding; Novartis: Research Funding; Celgene: Membership on an entity's Board of Directors or advisory committees; Teva: Membership on an entity's Board of Directors or advisory committees. Kolla:Amgen: Equity Ownership. Bachanova:Seattle Genetics: Membership on an entity's Board of Directors or advisory committees; Gamida Cell: Research Funding; Novartis: Research Funding; Kite: Membership on an entity's Board of Directors or advisory committees; Incyte: Research Funding; Celgene: Research Funding; GT Biopharma: Research Funding. Gerson:Abbvie: Consultancy; Seattle Genetics: Consultancy; Pharmacyclics: Consultancy. Barta:Janssen: Membership on an entity's Board of Directors or advisory committees; Celgene: Research Funding; Merck: Research Funding; Mundipharma: Honoraria; Bayer: Consultancy, Research Funding; Seattle Genetics: Honoraria, Research Funding; Takeda: Research Funding; Janssen: Membership on an entity's Board of Directors or advisory committees; Celgene: Research Funding; Mundipharma: Honoraria. Hill:Pharmacyclics: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; AstraZeneca: Consultancy, Honoraria; Celegene: Consultancy, Honoraria, Research Funding; Seattle Genetics: Consultancy, Honoraria; Takeda: Research Funding; Amgen: Research Funding; Kite: Consultancy, Honoraria; Gilead: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; TG therapeutics: Research Funding; Abbvie: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Genentech: Consultancy, Research Funding. Martin:Karyopharm: Consultancy; Sandoz: Consultancy; I-MAB: Consultancy; Celgene: Consultancy; Janssen: Consultancy; Teneobio: Consultancy. Danilov:Verastem Oncology: Consultancy, Other: Travel Reimbursement , Research Funding; Bristol-Meyers Squibb: Research Funding; Aptose Biosciences: Research Funding; Bayer Oncology: Consultancy, Research Funding; TG Therapeutics: Consultancy; Curis: Consultancy; Seattle Genetics: Consultancy; Celgene: Consultancy; MEI: Research Funding; Janssen: Consultancy; Abbvie: Consultancy; Pharmacyclics: Consultancy; Takeda Oncology: Research Funding; AstraZeneca: Consultancy, Research Funding; Gilead Sciences: Consultancy, Research Funding; Genentech: Consultancy, Research Funding. Grover:Seattle Genetics: Consultancy. Karmali:Takeda, BMS: Other: Research Funding to Institution; Astrazeneca: Speakers Bureau; Gilead/Kite; Juno/Celgene: Consultancy, Speakers Bureau. Ghosh:AstraZeneca: Honoraria, Speakers Bureau; Bristol-Myers Squibb: Honoraria, Speakers Bureau; Gilead: Consultancy, Honoraria, Speakers Bureau; Janssen: Consultancy, Honoraria, Research Funding, Speakers Bureau; Pharmacyclics LLC, an AbbVie Company: Consultancy, Honoraria, Research Funding, Speakers Bureau; SGN: Consultancy, Honoraria, Research Funding, Speakers Bureau; TG Therapeutics: Consultancy, Honoraria, Research Funding; Celgene: Consultancy, Research Funding; Genentech: Research Funding; Forty Seven Inc: Research Funding. Park:BMS: Consultancy, Research Funding; Rafael Pharma: Membership on an entity's Board of Directors or advisory committees; G1 Therapeutics: Consultancy; Teva: Consultancy, Research Funding; Gilead: Speakers Bureau; Seattle Genetics: Research Funding, Speakers Bureau. Epperla:Verastem Oncology: Speakers Bureau; Pharmacyclics: Honoraria. Hamadani:Pharmacyclics: Consultancy; Merck: Research Funding; Celgene: Consultancy; ADC Therapeutics: Consultancy, Research Funding; Sanofi Genzyme: Research Funding, Speakers Bureau; Janssen: Consultancy; Otsuka: Research Funding; Medimmune: Consultancy, Research Funding; Takeda: Research Funding. Kahl:BeiGene: Consultancy; TG Therapeutics: Consultancy; ADC Therapeutics: Consultancy, Research Funding; Seattle Genetics: Consultancy. Flowers:Gilead: Consultancy, Research Funding; BeiGene: Consultancy, Research Funding; AstraZeneca: Consultancy; Denovo Biopharma: Consultancy; National Cancer Institute: Research Funding; Genentech, Inc./F. Hoffmann-La Roche Ltd: Consultancy, Research Funding; Celgene: Consultancy, Research Funding; Millenium/Takeda: Research Funding; Bayer: Consultancy; AbbVie: Consultancy, Research Funding; V Foundation: Research Funding; Optimum Rx: Consultancy; Eastern Cooperative Oncology Group: Research Funding; Karyopharm: Consultancy; Burroughs Wellcome Fund: Research Funding; TG Therapeutics: Research Funding; Acerta: Research Funding; Pharmacyclics/Janssen: Consultancy, Research Funding; Spectrum: Consultancy. Cohen:LAM Therapeutics: Research Funding; Takeda Pharmaceuticals North America, Inc.: Research Funding; Gilead/Kite: Consultancy; Astra Zeneca: Research Funding; Genentech, Inc.: Consultancy, Research Funding; Janssen Pharmaceuticals: Consultancy; Seattle Genetics, Inc.: Consultancy, Research Funding; Bristol-Meyers Squibb Company: Research Funding; ASH: Research Funding; Lymphoma Research Foundation: Research Funding; Hutchison: Research Funding; UNUM: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal