

Background: Return to full-time work after hematopoietic cell transplant (HCT) is an important indicator of health recovery and overall function of survivors. Because young adult (YA) HCT patients are at a critical personal and professional developmental phase at the time of their illness, they face unique challenges potentially impacting their ability to work post-HCT. We aimed to assess the post-HCT work status of YA patients undergoing allogeneic HCT and examine pre-HCT factors associated with their work status at the 1-year time-point post-HCT.
Methods: Using data from the Center for International Blood and Marrow Transplant Research (CIBMTR), we studied YA (18-39 years of age at HCT) survivors (alive ≥1-year post-HCT) of allogeneic HCT performed between 2008 and 2015 for malignant or non-malignant conditions. All conditioning regimens, stem cell sources, and donor types were included. Work status [full-time (FT), part-time (PT), unemployed, medical disability] was assessed at 6-months, 1-, 2-, and 3-years post-HCT. We performed a multivariable logistic regression to study the pre-HCT patient and disease related [patient age at HCT, sex, race/ ethnicity, pre-HCT education, pre-HCT work status, disease diagnosis, Karnofsky/ Lansky performance score, hematopoietic cell transplant comorbidity index (HCT-CI), marital status], and HCT-related (year of transplant, stem cell source, donor type, conditioning regimen) factors associated with post-HCT work status at the 1-year time-point [dichotomized as employed (in FT/PT work) vs unemployed (unemployed, medical disability)].
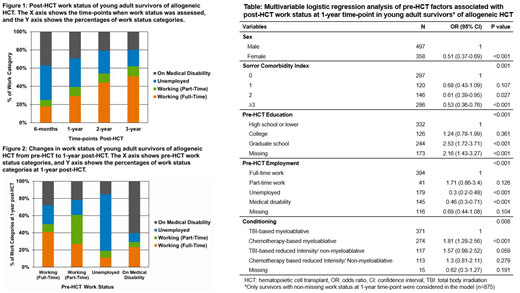
Results: A total of 1,365 allogeneic HCT recipients met the selection criteria. Median age at HCT was 30.8 years (range 18-39; interquartile range 9.3). Forty-four percent were females; 89% received HCT for malignant diseases (myeloid diseases: 62%, lymphoid diseases: 35%) and the remainder for non-malignant diseases (severe aplastic anemia, inherited abnormalities of erythrocyte differentiation/ function, and disorders of the immune system). Forty three percent received total body irradiation (TBI) based myeloablative conditioning regimens. Median follow-up time from HCT was 60.6 months (range: 12-121). From 6-months to 3-years post-HCT, the percentage of survivors employed FT (18% to 51%) and PT (7% to 11%) increased, and unemployed (38% to 18%) and on medical disability (37% to 20%) decreased (Figure 1). Of patients in FT work pre-HCT, 50% were either unemployed or had medical disability status at the 1-year time-point (Figure 2). Of those unemployed pre-HCT, 19% were working at 1-year post-HCT. In the multivariable logistic regression, survivors' pre-HCT work status was significantly associated with the post-HCT work status at 1-year time-point. Compared to patients working FT pre-HCT, patients who were unemployed and on medical disability were significantly less likely to be employed at 1-year post-HCT [pre-HCT unemployment: odds ratio (OR) of FT/PT employment 0.30; 95% confidence interval (CI) 0.20-0.48; pre-HCT medical disability: OR 0.46; 95% CI 0.30-0.71]. Females (OR 0.51; 95% CI 0.37-0.69) and patients with an HCT-CI score of 2 (OR 0.61; 95% CI 0.39-0.95), and ≥3 (OR 0.53; 95% CI 0.36-0.76) also had a lower likelihood of employment. Compared to patients with high school or lower education, patients with graduate school level education had significantly higher likelihood of employment (OR 2.53; 95% CI 1.72-3.71). Compared to patients treated with total body irradiation (TBI) based myeloablative conditioning, significantly higher odds of employment were seen in chemotherapy-based myeloablative conditioning (OR 1.81; 95% CI 1.28-2.56) (Table).
Conclusions: In YA HCT survivors, the full-time and part-time work rates steadily improved post-HCT. Nonetheless, nearly 40% were still either unemployed or on medical disability even at 3 years post-HCT. Although there were limitations of the study including lack of post-HCT time-dependent covariates for the analysis and direct patient report for work status, our study findings provide an insight into the factors impinging on YA survivors' ability of returning to work and points to a need for return to work interventions.
Shaw:Therakos: Other: Speaker Engagement.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal