

Adult T-cell leukemia/lymphoma (ATL) is a peripheral T-cell malignancy associated with the human T-cell leukemia virus type I (HTLV-1). Classification of ATL into clinical subtypes acute, lymphoma, chronic and smoldering types was proposed based on prognostic factors, clinical features and natural history of the disease. Although HTLV-1 infection alone is not sufficient to cause ATL and only about 5% of HTLV-1 carriers progress to ATL, the prognosis is generally poor especially for patients with aggressive ATL (i.e., acute, lymphoma or unfavorable chronic types), with a median survival time at around 1 year, even after chemotherapy. Currently, biomarkers to predict ATL onset and progression are limited, making early diagnosis and treatment for ATL challenging. To develop early diagnostic biomarkers for ATL, we performed, for the first time, an extensive proteomic profiling of HTLV-1 carriers and ATL patients as a foundation for establishing a blood-based biomarker panel for ATL.
Expression levels of 1305 plasma proteins in HTLV-1 carriers (n=40), untreated ATL patients (n=40, 28 acute; 4 lymphoma; 5 chronic; 3 smoldering), and remission status (n=5) were measured by SOMAscan assay (SomaLogic Inc, Boulder, CO). ATL diagnosis was based on criteria proposed by the Japan Clinical Oncology Group (JCOG) and identification of monoclonal integration of HTLV-1 proviral DNA using Southern blot hybridization method. Deregulated proteins in HTLV-1 versus ATL versus remission states were ranked by significance (Welch's t-test) and discrimination capacity (area under the curve [AUC]). In addition, machine learning algorithms were used to set discrimination boundaries for HTLV-1, ATL, and remission states using some of the top deregulated proteins. Statistical analyses were performed using Python 3.6.2 software. To elucidate on ATL pathogenesis, we further analyzed our proteomic data using Gene Set Enrichment Analysis (GSEA 3.0 hallmarks, curated gene sets) and Gene Ontology (GO Panther Pathways) and determined pathway deregulation among disease states as well as among ATL subtypes. Overrepresented pathways in ATL versus HTLV-1 included inflammation mediated by cytokine and chemokine signaling, angiogenesis, notch signaling, and IL6/JAK/STAT3, among others. Among a total of 176 proteins which were categorized as extremely significant (p<0.00001) with AUC scores ranging from 0.90-0.99, we further confirmed plasma protein concentrations of CD223 (LAG3) (n=40, 2 healthy individuals; 8 HTLV-1 carriers; 10 acute; 8 lymphoma; 6 chronic; 6 smoldering), CD30 (TNFRSF8), TIM-3 (HAVCR2) (n=40, 2 healthy individuals; 8 HTLV-1 carriers; 12 acute; 6 lymphoma, 6 chronic; 6 smoldering), and TNFR2 (TNFRSF1B) (n=79, 5 healthy individuals; 16 HTLV-1 carriers; 26 acute; 9 lymphoma; 11 chronic; 9 smoldering), through ELISA.
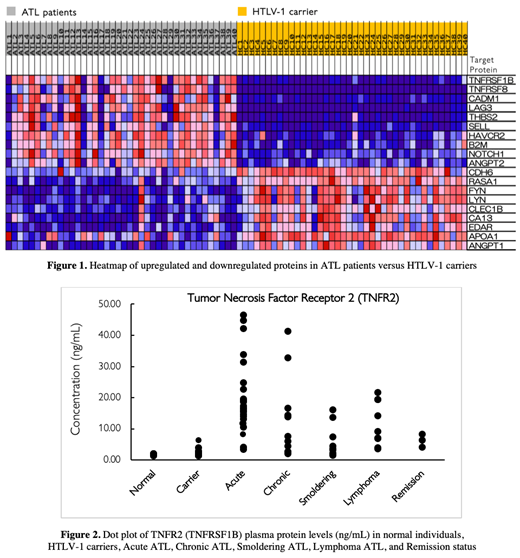
We discovered significantly higher CD30 and TIM-3 levels in acute ATL versus HTLV-1 carriers (p<0.05) and remarkably high TNFR2 levels among aggressive ATL patients, acute (p<0.001) and lymphoma types (p<0.01) versus HTLV-1 carriers. In addition, a significant decrease in TNFR2 levels among ATL patients who have achieved remission was also seen (p<0.001). These results indicate the potential value of TNFR2 not only as a diagnostic biomarker for ATL, but also for predicting response or failure to therapy. Furthermore, this study represents a novel proteomic approach in developing candidate biomarkers for ATL, by combining data from high-throughput SOMAmer technology, machine learning, proteomic pathway analysis, in addition to previously well-established techniques such as ELISA. Further investigation of TNFR2 and other potential biomarkers in this study need to be done in the near future.
Fukushima:Daiichi-Sankyo: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal