

Introduction
Steroids refractory (SR) acute (a) or chronic (c) graft versus host disease (GVHD) carries morbidity and lethality. Treatment algorithms varies widely among institutions meaning that the most effective treatment is not yet established. Extracorporeal photopheresis (ExP) and Ruxolitinib have shown in retrospective studies a hopeful efficacy in the treatment of this disease. Moreover, prolonged corticoid or immunosuppressant drugs are associated with opportunistic infection and mortality. Consequently our GVHD algorithm consider 7 days of high dose steroids before moving on to the second line treatments mentioned above to avoid prolonged infectious risk. Because of quick availability and reported benefit, without adding more immunosuppression, we have prefered ExP over other treatments. However this apparent advantages are contrasted with its great cost, as each session exceeds $US 2000. Ruxolitinib in the other hand, is less expensive, but since it is only administered orally, doubts regarding its absorption frequently appear in situations of intestinal GVHD. Hence we used Ruxolitinib as third line therapy after ExP. To know real outcomes of our patients we analyzed all patients with SR-GVHD of our adult hematopoietic transplantation program.
Methodology
Since 1993 we prospectively performed a registry of all transplanted patients. For this analysis we reviewed all allogeneic transplantated patients and data of those who developed SR-GVHD was extracted. In 2013, ExP was available in our center and was included in our algorithm. SR-GVHD was defined as patients that did not respond despite 5-7 of high dose steroids. As some patients suffer from aGVHD and cGVHD we analyse them separately for global response purpose. Considering that some events can affect more than one organ, when less than 3 organs were affected, we also analyse responses to each one of them separately. When 3 or more organs were affected we consider it as multisystemic affectation
Results
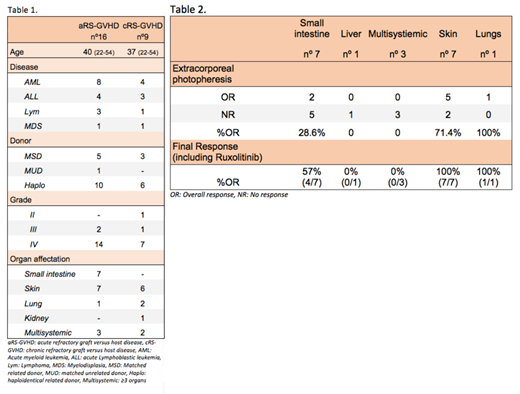
Until 2013 150 allogeneic transplants were performed; of those, 14 patients (9%) developed SR-GVHD, with 90% mortality. Unsuccessful treatmens included ATG, high doses of methylprednisolone, etanercept, and cyclosporine adjustment. Since 2013 we performed 135 allogeneic transplants and 20 patients (14,8%) developed SR-GVHD. Twelve patients presented with SR-aGVHD, 5 patients with SR-cGVHD and 4 patients with acute and chronic SR-GVHD in different time. For analysis of global response, then, we consider 16 SR-aGVHD patients and 9 SR-cGVHD patients (patients characteristics are shown in table 1). All 16 SR-aGVHD patients were treated with ExP with a median of 5,3 sessions. Among SR-aGVHD patients 37% responded to ExP, all being complete responses. When including ruxolitinib addition, final responses reached 56,3%. Mortality was high in this group (56,3% died, 66% of them because of aGVHD). In patients with no response to ExP and Ruxolitinib, mortality rate was 85,7%. Most affected organs were small intestine and skin, affecting 43,7% of patients each. Responses to therapy by organ affectation are shown in table 2. In SR-cGVHD, ExP was used in 7/9 patients, and 85,7% responded. In this case most patients only achieved partial response (71,4%) and ruxolitinib did not improved response any further. Among SR-cGVHD, skin affectation was the most common, 66% of SR-cGVHD patients presented with skin affectation either exclusively or combine with other organ affectation.
Conclusions
SR-GVHD remains a challenging disease, and no standard treatment exist. Beyond the high mortality rate, cost associated with treatment, procedures and hospitalization makes this patients even more difficult to manage. Therefore it is imperative that every center analyse their own data and treatment pathways to optimize both, GVHD treatment results and hospital resources. As a matter of fact, after reviewing our own data, we switched to a combined modality of ExP and Ruxolitinib for affectation other than skin, in SR- aGVHD. We hope this new algorithm overcomes, specially, the bad results of monotherapy in intestinal SR-aGVHD seen in our center, as these patients are exposed to high risk of malnutrition, dehydration, prolonged hospitalization and death. In SR-cGVHD we found a consistent tendency of partial responses with ExP.
Keywords: Steroids refractory graft versus host disease, Extracorporeal Photopheresis, Ruxolitinib.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal