

Introduction: Transfusion dependency in Myelodysplastic syndrome (MDS) patients is associated with shortened over-all survival and leukemia-free survival; however, it is not clear whether this detrimental effect is mediated by transfusional iron overload itself or whether the need for RBC transfusion is a surrogate marker of disease severity. Additionally, despite the negative effects of anemia and transfusion dependence on disease outcomes and patient quality of life, the clinical impact of iron overload in MDS remains controversial. Overall, the most common non-leukemic cause of death in MDS is heart failure. Recent T2* cardiac MRI (CMR) studies have shown that cardiac iron accumulation in MDS patients is variable and infrequent. T2* CMR is noninvasive, robust and the best available modality for assessing iron organ quantification.
The current study assessed iron overload in transfusion dependent MDS patients using ferritin levels combined with myocardial and liver iron quantification using T2* CMR. The study monitored iron accumulation dynamics while on iron chelation therapy.
Methods: We collected retrospectively clinical data in 18 RBC transfusion dependent MDS patients that had a CMR in our institution; some of the patients have serial scans. All scans were obtained using a 1.5 T scanner (Signa HDx ver 15 GE). Scans interpretation was performed using a dedicated workstation (Medis Medical imaging version 7.6, the Netherlands) for left ventricular ejection fraction measurement and T2* investigation as previously described. T2* values were recorded in milliseconds and converted to mg/gr dry tissue of myocardial liver and pancreatic tissue.
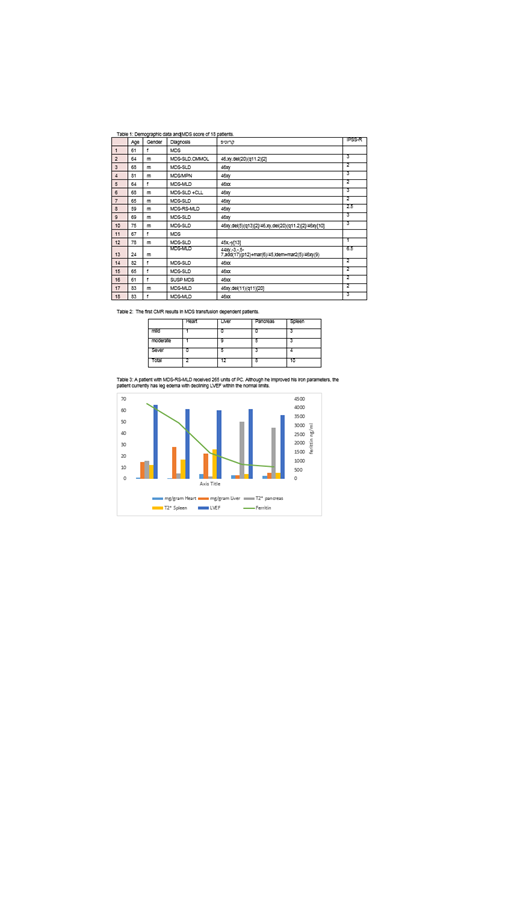
Results: Ten of 18 patients were chelated. During the study period 4 patients have died from pneumonia, brain tumor, complications of Allo BMT and transformation to AML. Demographic data and prognostic score of MDS are shown in table 1.
Before the first CMR, patients were treated with median of 48 PC (14-145) with median ferritin levels 1691.3ng/ml (269.4-3730ng/ml). In Table 2 we show iron accumulation in the first CMR. Iron accumulation in the heart was seen in 2 patients. The results are shown as severity of accumulation and not absolute numbers, as normal and abnormal range is different in the different organs.
Seven patients had yearly serial CMR done, 6 of them were treated with iron chelation. We found iron accumulation in the heart in 4 of them. In table 3 we show example of a patient that was treated with chelation.
Another patient, that had decrease ejection fraction with only moderate accumulation in the heart in CMR, improved her heart function with chelation.
During the study period all patients continue to be transfusion dependent except 1 patient that became transfusion independent. She was transfused with 182 PC with maximal ferritin of 6926ng/ml. She was chelated with deferiprone and then with desferal. She is now transfusion independent for a year.
Conclusion: Blood transfusion dependency in MDS patients, leads to high ferritin levels and evidences in CMR of iron accumulation in parenchymal orangs including the heart. During the study 4 patients had evidence of iron accumulation in the heart with 2 of them with severe accumulation that improved with iron chelation. Liver and pancreas accumulation was seen in 12 and 8 patients accordingly. Prospective studies documenting the correlation between chelation therapy and improvement in organ damage and survival are needed.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal