

Background
NK/T -cell lymphoma (NK/TCL) is a type of non-Hodgkin lymphoma common in México; however, there are few clinical studies of prevalence and clinical characteristics in non-Asian population. The objective was to identify the response to first line treatment in patients with NK/TCL and determine overall survival (OS) and disease-free survival (DFS).
Methods
We conducted a retrospective study from April 2006 to December 2018; clinical information was collected from electronic medical records from patients with NK/TCL without prior treatment. Pearson Chi-square tests were used to compare categorical variables, and t-test for quantitative variables. The Kaplan-Meier was used to determine OS and DFS. A bivariate analysis of factors that could influence OS and DFS was performed. Data analysis was done using the SPSS 23 statistical program.
Results
We included 173 patients with NK/TCL and complete clinical information. Male predominance was 1.8:1, median age 40 years old (16-85). Nasal type lymphoma occurred in 90.2% of cases and extranasal in 9.8%.The most frequent location site was nose (69%), follow by palate (15%), pharynx, larynx and Waldeyer´s ring (6.4%), skin and soft tissues (5.2%). At diagnosis, 68% were in ECOG<2 and 69% had B symptoms. More than 60% of cases presented as early clinical stages (stage I 35%, stage II 30.4%, stage III 5.3% and stage IV 29.2%). In advanced stages, the most frequent sites of infiltration were CNS (30%), skin and soft tissue (22%), intestine and lung (18%), bone marrow (<10%). The elevation of LDH as well as β2 micro globulin was reported in 44.4% and 50.7%, respectively.
We applied four prognostic scales (IPI, K-IPI, PINK and PINK-β); regardless which one we used, more than 50% of patients presented a low risk, with the exception of stratification with the K-IPI scale, where more than 50% corresponded to an intermediate to risk.
Nineteen patients did not receive treatment (due to scarce economic resources) and, in two patients, it was not possible to assess the response to treatment. We analyze 152 cases; monotherapy was administrated in 42.4% (38.4% received radiotherapy (RT), while 61.6% received only chemotherapy (CT)). The 57.8% received combined therapy (CT+RT). The modalities used were sequential (58%), sandwich (26%) and concurrent treatment (16%). The chemotherapeutic regimens used were divided into three groups chemotherapy anthracycline based therapy (CHOP: 38%), with L-asparaginase (48%) and others (14%).
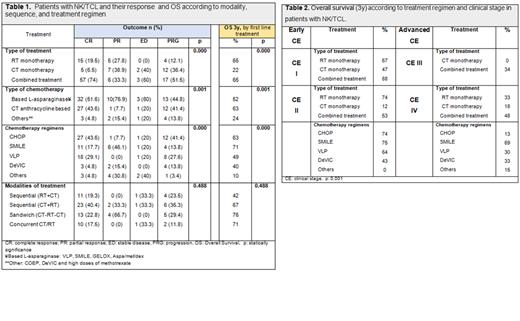
Of the entire population at the end of the study, 50.7% achieved complete response (CR), 11.8% partial response (PR), 3.3% stable disease (SD), 21.7% progression and 12.5% had died. Sixty-four percentage of patients who received combined therapy achieved CR. Outcome, as progression and death were more frequent in patients receiving only CT, 30.7% and 33.3%, respectively. CR greater than 50% was found with VLP and CHOP; meanwhile progression is less common with the use of SMILE (17.4%) (Table 1).
The 3-year OS was 52% with a median follow-up of 3.6 years. The type of treatment, type of chemotherapy and chemotherapy regimens had a statistically significant impact (Table 1). In early stages OS was greater than 50% with CT+RT and with only RT. The 3-year OS was less than 50% in advanced stages regardless of the type of treatment however, the use of SMILE improves OS (3y) to 69% (Table 2). The scales that allow a greater separation between high or low risk groups were IPI and K-IPI, and have an impact on OS (p = 0.000).
The 3-year SLE was 49%, with a median follow-up of 2.6 years, in this case only the type of treatment had a statistically significant influence (p 0.000). SLE (3y) with CT + RT was 58% vs 6% with RT and 0% with CT.
Mortality was 45.7%, the most frequent cause of death was infection during treatment (85%) followed by disease activity (15%). Fifty-four percent is alive, 43% of them in RC.
Conclusions
NK/TCL lymphoma predominated in our male patients of productive age and in advanced clinical stages. The prognosis had greater clinical impact with the use of IPI and K-IPI scores. In early clinical stages, patients should receive radiation therapy and consider chemotherapy (VLP). In advanced stages, combined treatment is required, with the use of L-asparaginase chemotherapeutic regimens (like SMILE).
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal