

The first and second authors contributed equally to this publication.
Background: Tisagenlecleucel is a CD19-directed autologous chimeric antigen receptor (CAR)-T cell therapy approved for the treatment of patients (pts) up to 25 years of age with B-cell acute lymphoblastic leukemia (ALL) that is refractory or in ≥ 2nd relapse. However, pts < 3 years of age at screening were excluded from tisagenlecleucel clinical trials in relapsed/refractory (r/r) ALL (NCT02435849 [registrational ELIANA] and NCT02228096 [ENSIGN]). Here we present tisagenlecleucel manufacturing experience in pts < 3 years of age with r/r ALL in the commercial setting since regulatory approval.
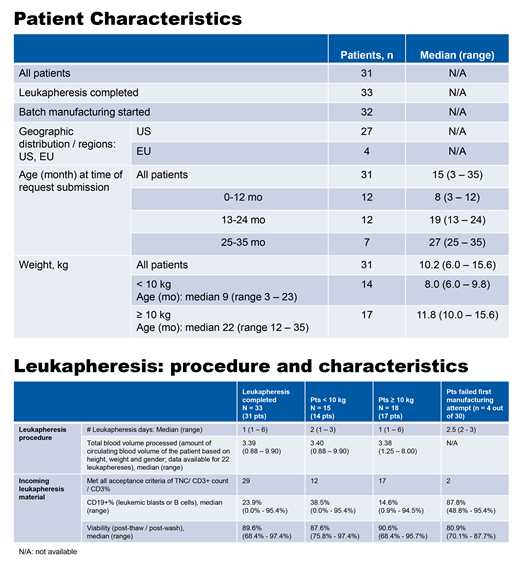
Methods: Eligible pts were < 3 years of age at time of the request for commercial tisagenlecleucel, with manufacturing data after August 30, 2017 (first FDA approval of tisagenlecleucel). Tisagenlecleucel was manufactured at Morris Plains, NJ, USA. Patient leukapheresis and manufacturing outcome data are presented for all patients and stratified by weight (< 10 kg and ≥ 10 kg).
Results: Among 31 pts, the median age was 15 months (range, 3-35) and median body weight 10.2 kg (range, 6.0-15.6) at leukapheresis (14 pts < 10 kg and 17 pts ≥ 10 kg). Thirty-three leukaphereses were performed in 31 pts (Table 1; 2 pts underwent repeat leukapheresis for second manufacturing attempt), with a median of 1 leukapheresis day required to meet adequate cell counts (range, 1-6; Table 2). The acceptance criteria for tisagenlecleucel manufacture (total nucleated cells [TNC], CD3+ cells, CD3+% of TNC) were met in 29/33 leukapheresis materials; 2/3 that did not meet acceptance criteria were unsuccessful. Following the first manufacturing attempt in 30 pts (1 pt has not yet started manufacture), 26/30 (86.7%) were successful and 4/30 experienced manufacturing failure (2 pts < 10 kg and 2 pts ≥ 10 kg). Manufacturing success is defined as formulation of a final product (FP) within approved release specifications. Of the 4 manufacturing failures, 2 successfully underwent repeat leukapheresis and remanufacturing on second attempt and 2 did not undergo a second attempt. For 2 of the 4 manufacturing failures, the leukapheresis material did not meet acceptance criteria (pts were unable to undergo additional days of leukapheresis). The median manufactured cell dose in FP was 4.0x106 CAR+ viable T cells/kg (range, 0.37x106 -4.0x106), median % cell viability was 87.6% (range, 66.7%-95.7%), and median CAR+% expression was 10% (range, 2.7%-25.6%). Based on interaction with site personnel, measures to optimize leukapheresis in young pts with low weight, particularly < 10 kg, appeared to be essential, including raising hematocrit to 40% with blood transfusion, appropriate size central venous catheter, blood prime of the apheresis instrument, prevention of hypothermia during collection, close monitoring of vital signs and electrolytes, partial rinse back, and allowing > 1 day of leukapheresis to meet acceptance criteria.
Conclusions: Leukapheresis and tisagenlecleucel manufacturing in pts with r/r ALL < 3 years of age and low weight (as low as 6 kg and as young as 3 months) are feasible and do not present manufacturability risk compared to Novartis clinical trial experience in patients ≥ 3 years of age.
Eldjerou:Novartis Pharmaceuticals Corporation: Employment. Acker:Novartis: Employment. Howick:Novartis: Employment. Clough:Novartis: Employment. Fuchs:Novartis: Employment. Salmon:Novartis: Employment. Willert:Novartis: Employment. Tiwari:Novartis: Employment. Pujols:Novartis: Employment. Robson:Novartis: Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal