

Introduction:
Hemophagocytic lymphohisticoytosis (HLH) is a life threatening disorder resulting from uncontrolled macrophage activation. HLH may be primary or associated with active infection, autoimmune disorder or neoplasia. In a recently reported national surveillance report from the Food and Drug Administration (FDA), HLH was observed shortly after the initiation of lamotrigine (Lamictal®) in eight patients. We report the development and treatment of HLH in an otherwise healthy young woman who was briefly treated with lamotrigine.
Case:
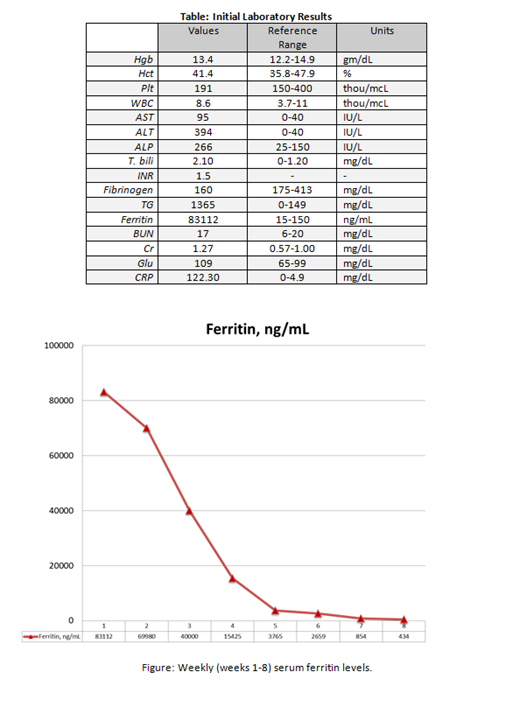
A 27 year-old female with a history of bipolar depression and anxiety began treatment with lamotrigine 25 mg daily. Six days later, she experienced cough and odynophagia progressing to nausea, vomiting, and diarrhea over one day. She was treated with cephalexin for presumptive streptococcal pharyngitis by her primary physician. The next morning she developed diffuse rash, along with lethargy, myalgia, dyspnea and headache, and presented to the emergency room. Vital signs revealed tachycardia, tachypnea, hypoxia, and fever. Her exam was significant for decreased alertness, and pulmonary rhonchi with wheezing. A lumbar puncture displayed cerebrospinal fluid pleocytosis. Liver function tests were abnormal with elevated transaminases and hyperbilirubinemia, and ferritin was markedly elevated. In addition, serum creatinine, C-reactive protein, triglycerides and prothrombin time were elevated [Table]. Rash and overall rapid decline without clear etiology prompted concern for HLH. Lamotrigine was discontinued and a bone marrow biopsy was obtained and revealed normocellular marrow with relative myeloid hyperplasia with erythroid hypoplasia and increased histiocytes without evident hemophagocytosis.
Our patient was initially treated with several broad spectrum antibiotics, including vancomycin, meropenem, acyclovir, and clindamycin. Due to worsening oxygenation and respiratory failure, she was intubated. Low-grade disseminated intravascular coagulation developed requiring two units of cryoprecipitate. Intravenous immunoglobulin G (1 gm/kg daily) was administered on hospital days 3 and 4 along with five days of pulse dose steroids (30 mg/kg). On hospital day 9, as her respiratory status worsened she was placed on venous-venous extracorporeal membrane oxygenation (VV ECMO).
Treatment with etoposide (300 mg twice weekly - dose adjusted to account for extracorporeal blood volume) and dexamethasone (10 mg/m2 daily) per HLH protocol was initiated. Neutropenia developed after two doses of etoposide, and was subsequently held. The patient remained on VV ECMO for eight days, and was able to be extubated on hospital day 18. Liver and renal function improved, and ferritin level progressively declined over the course of the admission, to near normal at discharge [Figure]. She was discharged on hospital day 32 and is currently living independently at home.
Discussion:
Our patient was admitted with overwhelming illness, requiring intensive management. She met diagnostic criteria for HLHand once stable, was treated per guidelines of HLH-94 protocol.
The month prior to her presentation, a report from investigators at the FDA (Kim T, et al, Neurology 2019;92 e2401-5) using the Adverse Event Reporting System described eight cases of HLH associated with lamotrigine. In light of this report, we describe another patient with HLH developing in a temporal relationship with lamotrigine and in absence of other identifiable causes. The patient was diagnosed with HLH based on H score probability of 94%. Similar to those cases in the FDA report, the syndrome developed shortly after starting lamotrigine and improved after stopping therapy. Lamotrigine is a widely prescribed for bipolar disorder, and increasingly for depression. Other adverse reactions associated with lamotrigine include Stevens-Johnson syndrome, toxic epidermal necrolysis and drug reaction with eosinophilia and systemic symptoms. It should be stated that these conditions cannot be excluded in this case, as they represent a similar over activation of the immune system with manifestations that overlap with HLH.
Early identification and intervention are critical for the successful treatment of HLH. In addition to stopping lamotrigine, immunosuppressive therapy may be beneficial. Presently, there are no guidelines that specifically address treatment for drug-induced HLH.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal