

Ibrutinib (Ibr) is a specific inhibitor of Bruton tyrosine kinase, a component of the B-cell receptor (BCR) signaling. Venetoclax (Veneto) inhibits the anti-apoptotic protein BCL2. Both drugs are highly effective as monotherapy against chronic lymphocytic leukemia (CLL) (Byrd NEJM, Roberts, NEJM, 2015 and Roberts, Blood, 2019) and clinical trials using the combination therapy are ongoing. An interesting clinical observation is that the tumor cell sensitivity to these two drugs differ between different anatomic compartments. While lymph node-resident CLL cells are more sensitive to ibr, circulating CLL cells in the peripheral blood are more sensitive to the action of veneto. When these two drugs are used in combination to treat relapsed/refractory (Hillman ASH 2018 and Kater EHA 2019) or previously untreated CLL patients (Jain NEJM 2019), rate of complete response significantly increases compared to single drug alone. Moreover, negativity of bone marrow minimal residual disease continues to improve over time.
However, the reason behind these observed compartmental responses is largely unknown, and we investigated the differential response using an ex vivo model that promotes CLL proliferation (CLL proliferation model). A better understanding of how these two drugs synergize would eventually help develop other rational combination strategies. We established the ex vivo model using fibroblasts derived from the bone marrow of a CLL patient. In this model, CLL cells closely interact with the bone marrow fibroblasts (BMF) (Fig.1) and divide and proliferate for several generations, as measured by CFSE labeling. The culture, in some cases, may continue for 10 weeks before cell death ensues. With this ability to promote long-term cell proliferation, the model recapitulates one of the most salient features observed histologically in the "proliferation centers" of the CLL lymph nodes.
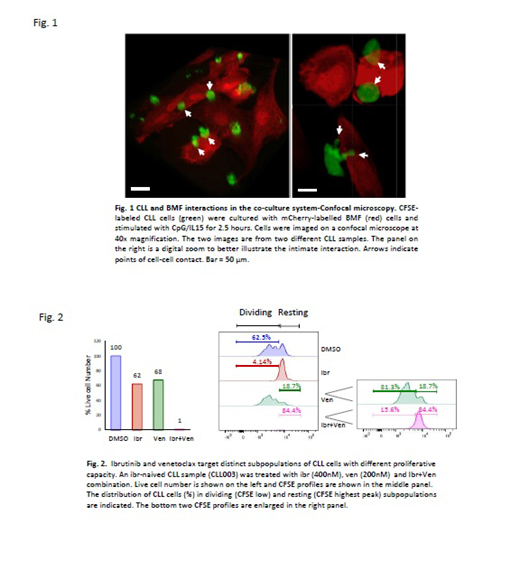
With the proliferation model, we first tested the effects of ibrutinib on cell division/proliferation as well as cell viability in samples taken from 30 CLL patients consisting of 22 ibr-naïve (thus sensitive) and 8 ibr-relapsed (thus resistant) patients. We demonstrate that there was lack of a significant inhibition of ibr on cell viability. In comparison, Ibr markedly inhibited cell proliferation in cells from ibr-naïve/sensitive patients (p<0.0001), while such inhibition was much less prominent in cells from ibr-relapsed/resistant patients (p=0.053). Overall, our data demonstrate that only the dividing subpopulation of CLL responds to ibr, and this response is highly correlated with patients' clinical response to the drug while cell viability responses are not.
With the CLL proliferation model, we also evaluated how veneto works. Veneto, as expected, markedly decreased cell viability at clinically achievable concentrations. CFSE profiles of the remaining live cells, however, revealed an interesting pattern of distribution, showing that veneto induces cell death but it preferentially kills the resting CLL population (Fig. 2). In other words, the resting subpopulation of CLL, instead of the dividing one, preferentially responds to veneto as compared to ibr.
Combination of the two drugs, as expected, worked most effectively, significantly reducing the total number of live cells, both resting and dividing subpopulations, in all cases. Analyses of CFSE profiles became less meaningful in many of these cases due to the small number of live cells remaining after the combination treatment.
In conclusion, our study, comparing the actions of ibr and veneto in a clinically relevant CLL proliferation model, demonstrates for the first time that the drugs target distinct subpopulations of CLL cells with different proliferative capacity. The data also suggest that single drug therapy may leave a subpopulation behind that would potentially rise to cause a future relapse. Our study provides a strong laboratory rationale explaining why combining these two drugs has the potential to eradicate CLL disease. The findings are also in line with the clinical observations regarding the compartmental response; ibrutinib works primarily on the lymph nodes where CLL cells divide in the "proliferation centers" and veneto acts preferentially on the circulating CLL cells that are mostly non-dividing and resting.
Wang:Incyte Reaserch Institute: Employment. Ma:Abbvie: Research Funding; Xeme: Research Funding; Novartis: Research Funding; Bioverativ: Consultancy; Janssen: Consultancy, Speakers Bureau; Beigene: Research Funding; Kite: Consultancy; Gilead: Research Funding; Pharmacyclics: Consultancy, Research Funding, Speakers Bureau; Acerta: Research Funding; Astra Zeneca: Consultancy, Research Funding, Speakers Bureau; Genentech: Consultancy; Incyte: Research Funding; Juno: Research Funding. Larson:Celgene: Consultancy; Agios: Consultancy; Novartis: Honoraria, Other: Contracts for clinical trials.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal