

Background: With the introduction of the Oncology Care Model, which aims to provide higher quality, more coordinated oncology care at the same or lower cost to Medicare, physician practices are increasingly being held accountable for performance and financial measures.1 Urgent care (emergency room [ER] visits and hospitalizations) is known to contribute a significant proportion of healthcare costs, and while there has been a focus on drug costs, little is known about the utilization or economic impact of urgent care among multiple myeloma (MM) patients.
Objective: To identify the primary reasons and economic burden of ER visits and hospitalizations among newly diagnosed MM (NDMM) patients during first line of therapy (LOT1).
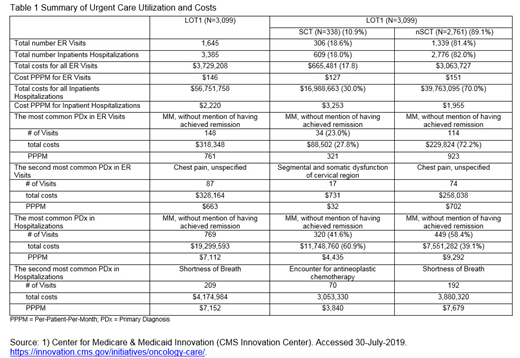
Methods: Patients from the Optum Clinformatics Extended DataMart - Date of Death database (Optum DOD) with ≥1 medical or pharmacy claim for an NCCN listed MM treatment from 7/1/11 to 3/31/2018 (index date) were included if they had diagnosis code for MM (ICD9/10 code 203/C90) and ≥6-months continuous enrollment without MM treatment prior to index date. Patients were followed until death, end of eligibility, or end of study (9/30/2018), whichever occurred first. The top 20 most common primary diagnoses (PDx) for ER visits and for hospitalizations were identified separately for patients who received stem cell transplant (SCT) or not (nSCT) during LOT1. Total costs and per-patient-per-month (PPPM) costs of ER visits and hospitalizations for each PDx were reported.
Results: Total 3,099 patients met inclusion criteria, including 2,761 (89.1%) nSCT and 338 (10.9%) SCT patients. nSCT patients were older than SCT patients (median nSCT=72 years vs SCT=62 years, p < 0.0001). The most common treatment regimens among nSCT were bortezomib in combination with dexamethasone (dex) (34%) followed by lenalidomide in combination with dex (27.4%). The most common treatment regimen among SCT were bortezomib in combination with lenalidomide and dex (46%) followed by bortezomib in combination with chemotherapy (18.3%). Median duration of LOT1 was 5.1 months among all patients, with median 11.2 months among SCT vs 4.5 months among nSCT, p < 0.0001). Among all patients, (Table 1) there was a total of 1,645 ER visits and 3,385 hospitalizations with a total cost of $3,729,208 and $56,751,758, respectively, and a PPPM cost of $146 and $2,220 for ER visits and hospitalizations, respectively. Among nSCT, there were 1,339 (81% of the total) ER visits and 2,776 (82% of the total) hospitalizations with a total cost of $3,063,727 and $39,763,095, respectively, and a PPPM cost of $151 and $1,955 for ER visits and hospitalizations, respectively. Among SCT, there were 306 (19% of the total) ER visits and 609 (18% of the total) hospitalizations, with a total cost of $665,481 and $16,988,663, respectively, and a PPPM cost of $127 and $3,253 for ER visits and hospitalizations, respectively. The most common PDx for hospitalizations among the entire cohort was 'MM, without mention of having achieved remission' with 769 hospitalizations for a total cost of $19,299,593 and a PPPM cost of $7,112. This same PDx was the most common among nSCT with 449 (58%) hospitalizations for a total cost of $7,551,282 and a PPPM cost of $9,292; as well as for SCT with 320 (42%) hospitalizations for a total cost of $11,748,760 and a PPPM cost of $4,435. This was also the most common PDx for ER visits among nSCT and SCT. For hospitalizations, the second most common PDx among the entire cohort and among nSCT was 'shortness of breath' while for SCT it was 'administration of antineoplastic chemotherapy'. The second most common PDx overall and for nSCT for ER visits was 'chest pain' and for SCT patients was 'musculoskeletal dysfunction (Segmental and somatic dysfunction of cervical region)'.
Conclusions: In this analysis, NDMM patients experienced frequent ER visits and hospitalizations over a median of ~5 months for a total cost of more than $60 million, with most of the cost among nSCT patients. The most common PDx was related to MM. Even though some hospitalizations for the SCT patients may have been for the SCT procedure itself, the economic burden of urgent care for MM patients remains very high. Additional research to assess the impact of newer treatments on urgent care visits among NDMM, identify patients at high risk of urgent care visits may provide insight into the potential for developing cost-saving interventions to reduce the utilization of urgent care.
Maiese:Janssen: Employment, Equity Ownership. Zhu:Janssen Scientific Affairs, LLC: Other: contractor for Janssen. Wu:Janssen: Employment, Equity Ownership. Chen:Janssen: Employment, Equity Ownership. Ailawadhi:Janssen: Consultancy, Research Funding; Takeda: Consultancy; Celgene: Consultancy; Cellectar: Research Funding; Amgen: Consultancy, Research Funding; Pharmacyclics: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal