

INTRODUCTION
The t (11; 14) by fluorescent in situ hybridization (FISH) is found in 15-20% of patients with multiple myeloma (MM) . Although it was classically considered a standard risk translocation or even a good prognosis, recent studies conducted in the era of new drugs show contradictory results and it is not well established if they have to be considered intermediate or standard risk.
The possibility of using targeted therapy with venetoclax for patients harboring t(11;14) makes the investigation of the outcome of newly diagnosed multiple myeloma (NDMM) with t(11;14) as relevant.
METHODS
We analyzed the baseline characteristics and outcome of patients with t(11;14)and receiving HDT-ASCT within the series of 647 patients with NDMM between 1988 and 2018 according to the current criteria at each moment at two academic hospitals in Spain (University Hospital of Salamanca and Hospital of Leon) . The FISH was performed on selected cells according to international regulations and centralized at the University Hospital of Salamanca.
For this purpose, a descriptive cross-sectional study was first conducted comparing the characteristics of patients with t (11; 14) versus the rest. The final objective wasto evaluate the role of HDT-ASCT in NDMM with t(11;14).
RESULTS
The baseline characteristics of the whole series were: a median age of 71years (yrs) (range:30-96). 217 patients (33,5%) were under 65 years. 352 (56.2%) were IgG; 161 (25.7%) IgA; 87 (13.9%) Bence Jones; 19 (3%) non-secretors, and 5 and 2 cases were IgD and IgM, respectively. 320 (53.2%) received novel agents as part of the first line of therapy. Overall, 153 (27.8%) achieved complete response (CR) after first line, and 403 (73.1%) at least a partial response.
After a median follow-up for living patients of 4.26 yrs (range: 0,1-27.3), the OS of the entire series was 2.74 years.
T(11;14) was performed in 440 NDMM patients and was positive in 80 (18.2%). Only in 5 patients other high-risk alterations (t (14:16), t (4:14) or del17p (p53)) were detected.
The baseline characteristics of patients with and without t (11:14) did not show significant differences, except for the heavy chain pattern(p <0,001). IgA was lower in patients with t(11:14) 12,8% (10 out of 78)vs 27,7% (98 out of 353).
Of note, most patients with non-secretory MM (10 out of 16, 62,5%) had the t(11;14) whilst in the conventional secretory MM patients, t(11;14) was observed in 68out of 415(16,4%). In addition, the plasma cell bone marrow infiltration was significantly higher in patients with t(11;14)(> 60% Plasma Cells) 32.8% vs 13.3%(p <0.001)).
HDT-ASCT was performed in 162 patients (25%)and 22 of them (13,5%) were positive for the t(11:14) and only in 2 patients, other high-risk alterations were detected.The induction therapy received in both treatments arms was homogeneous basically consisted on combinations of proteasome inhibitors plus immunomodulatory drugs.
The median OS for NDMM patients undergoing ASCT was 4,33 years. (range: 0,47-26,85) and the median PFS for this patients was 2,25 yrs (range: 0,1-27,25)
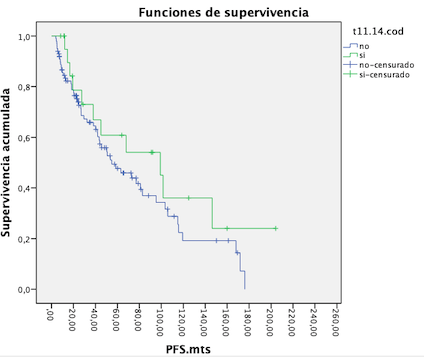
The median PFS for patients with t (11/14) undergoing ASCT trended to be higher than that observed in patients without t(11;14) who received also HDT-ASCT (99.1 vs 54.9 months), without obtaining significant results, (p 0.205) maybe due to the small number of patients (Figure 1).The median OS in the group of patients with and without t(11:14) undergoing ASCT was 120,8 vs 140 months (p= 0,829).
In the cohort of non eligible ASCT patients both median PFS and OS for patients with t(11:14) was similar than that observed in patients without t(11:14)(median PFS of 19,9 vs 19,4 months) (p 0,438) and (median OS of 31,5 vs 44 months) (p 0,424), respectively.
CONCLUSION
T(11;14) seems to be a cytogenetic abnormality more frequently observed in patients with NDMM and non secretory phenotype what requires further investigation. Patients with t(11;14) benefit the most if they received HDT-ASCT and it would represent a therapeutic strategy of choice if the patient is transplant-eligible.
Puig:Celgene: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Janssen: Consultancy, Honoraria, Research Funding; The Binding Site: Honoraria; Takeda, Amgen: Consultancy, Honoraria. Mateos:Abbvie: Membership on an entity's Board of Directors or advisory committees; GSK: Membership on an entity's Board of Directors or advisory committees; Pharmamar: Membership on an entity's Board of Directors or advisory committees; Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees; Takeda: Honoraria, Membership on an entity's Board of Directors or advisory committees; Adaptive: Honoraria; EDO: Membership on an entity's Board of Directors or advisory committees; Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal