

Introduction
Minimal residual disease (MRD) status at day 100 following autologous stem-cell transplant (ASCT) in multiple myeloma (MM) patients is an important determinant of prognosis. Bone marrow (BM) based assays, i.e. next-generation flow cytometry (NGF) or next-generation sequencing (NGS) that are currently used in determining MRD are vulnerable to sampling biases due to patchy marrow involvement and extramedullary disease. BM examination alone may lead to false-negative results. MRD assessment through newer, more sensitive peripheral blood based methodologies such as mass spectrometry (MS) can potentially overcome the limitations associated with BM based assays. At our institution, traditional immunofixation electrophoresis (IFE) has been replaced by a MS method termed Mass-Fix which utilizes the unique light chain mass associated with each patient's monoclonal protein to monitor disease over time. In this study, we assessed the prognostic impact of serum Mass-Fix MRD status in MM patients who were MRD negative by NGF around day 100 post-ASCT.
Methods
Patients with MM who underwent ASCT between 01/01/2015 and 12/31/2018 at Mayo Clinic, Rochester were included in this study provided they had attained post ASCT day 100 complete response (CR) by IMWG 2016 criteria and MRD- state as assessed by BM based NGF, utilizing 2 eight-color tubes (total 10 colors), with a minimum sensitivity 10-5. Presence of non-secretory MM and unavailability of pre-ASCT serum samples or serum IFE results were important exclusion criteria. Peripheral blood samples drawn concurrently with the BM assessment were evaluated by Mass-Fix as described previously (Mills et al., Clin. Chem, 2016). The isotype and mass of the M-protein light chain (LC) obtained by Mass-Fix were compared to the pre-ASCT M-protein LC and/or IFE isotype. Patients with the following genetic alterations: deletion 17p, translocation (4;14), (14;16), t(14;20) and1q gain/amplification and were considered high risk. All time-to event analyses were performed on JMP 14.1.0 from the time of ASCT using the Kaplan-Meier method.
Results
Sixty-two patients with MM (57 newly diagnosed and 5 relapsed/refractory) who underwent ASCT and were MRD- by BM based NGF around day 100 (range: day 60-120) were included in the study. Median age at ASCT was 61 (range: 40-76) years and 61% were males. Thirty (48%) patients had IgG MM, 15 (25%) patients had IgA MM and 17 (27%) patients had light chain only disease. Forty-one (66%) patients received bortezomib, lenalidomide and dexamethasone (VRD) as induction regimen. Median time from diagnosis to ASCT was 6 months (IQ range: 4.7-7.2). Pre-ASCT fluorescence in- situ hybridization data were available on 47 (76%) patients; 23 (49%) were high risk.
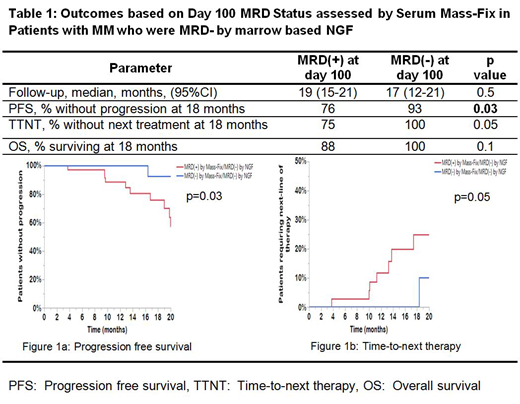
Of 62 patients, all of whom were day 100 MRD- by NGF, 36 (58%) patients had Mass-Fix identified MRD (MRD+). MRD positivity by Mass-Fix around day 100 was observed in 70% of patients with high risk MM versus 71% of patients with standard risk MM, p=0.9. The median follow-up was 18 months (95%CI: 14-21); 19 months (95%CI: 15-21) for patients who were MRD+ by Mass-Fix versus 17 months (95%CI: 12-21) for those who were MRD- by Mass-Fix at day ~100, p=0.5. Of 57 (92%) patients who received post ASCT maintenance therapy, 32 (89%) were MRD+ and 25 (96%) were MRD- by Mass-Fix, p=0.5.
Eighty-seven percent of patients with IgG MM had MRD+ status by Mass-Fix at day~100. By contrast, only 33% and 30% of patients with IgA MM and light chain MM, respectively, had MRD+ status at day 100; p<0.0001. This suggests that IgG half-life which is longer than that of IgA or free light chains may affect the day 100 MRD status. At 18 months, 76% and 93% of patients, who were MRD+ and MRD- , respectively by Mass-Fix were alive and free from disease progression, p=0.03 (Table 1, Figure 1a). At 18 months after ASCT, none of the patients who were MRD- by Mass-Fix required salvage treatment following ASCT while 25% of patients who were MRD+ by Mass-Fix required next line of therapy due to disease progression, p=0.05 (Table 1, Figure1b).
Conclusion
Our data suggest that outcomes [progression free survival (PFS) and time-to-next therapy (TTNT)] of patients with MM who are in CR, and have achieved MRD- state by BM NGF post ASCT, can be adversely impacted if there is concurrent evidence of serum monoclonal protein by Mass-Fix, thereby demonstrating incremental prognostic value of this sensitive assay in clinical practice.
Murray:The Binding Site: Patents & Royalties: US Patent Rights on Mass Spectroscopy Licensing agreement with The Binding Site, Research Funding. Dispenzieri:Akcea: Consultancy; Intellia: Consultancy; Janssen: Consultancy; Pfizer: Research Funding; Takeda: Research Funding; Celgene: Research Funding; Alnylam: Research Funding. Dasari:The Binding Site: Patents & Royalties: US Patent Rights on Mass Spectroscopy Licensing agreement with The Binding Site, Research Funding. Gertz:Teva: Speakers Bureau; Alnylam: Consultancy; Prothena Biosciences Inc: Consultancy; Janssen: Consultancy; Spectrum: Consultancy, Research Funding; Annexon: Consultancy; Appellis: Consultancy; Johnson and Johnson: Speakers Bureau; DAVA oncology: Speakers Bureau; Celgene: Consultancy; Research to Practice: Consultancy; Abbvie: Other: personal fees for Data Safety Monitoring board; Physicians Education Resource: Consultancy; Medscape: Consultancy, Speakers Bureau; Springer Publishing: Patents & Royalties; Amyloidosis Foundation: Research Funding; International Waldenstrom Foundation: Research Funding; Pharmacyclics: Membership on an entity's Board of Directors or advisory committees; Amgen: Consultancy; Ionis/Akcea: Consultancy; Proclara: Membership on an entity's Board of Directors or advisory committees; i3Health: Other: Development of educational programs and materials. Dingli:Karyopharm: Research Funding; Millenium: Consultancy; Rigel: Consultancy; Janssen: Consultancy; alexion: Consultancy. Lacy:Celgene: Research Funding. Leung:Omeros: Research Funding; Aduro: Membership on an entity's Board of Directors or advisory committees; Prothena: Membership on an entity's Board of Directors or advisory committees; Takeda: Research Funding. Kumar:Celgene: Consultancy, Research Funding; Janssen: Consultancy, Research Funding; Takeda: Research Funding. Kapoor:Takeda: Honoraria, Research Funding; Janssen: Research Funding; Celgene: Honoraria; Sanofi: Consultancy, Research Funding; Amgen: Research Funding; Glaxo Smith Kline: Research Funding; Cellectar: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal