

Background
In patients (pts) with chronic lymphocytic leukemia (CLL), tumor lysis syndrome (TLS) is a rare, but potentially life-threatening event. TLS is characterized by cytolysis leading to hyperkalemia, hyperphosphatemia, hyperuricemia and/or hypocalcemia, as defined by the Howard criteria. Analyses of patients (pts) treated with venetoclax monotherapy have reported TLS frequencies of up to 5%. In the CLL14 study, in which elderly, unfit pts were randomized to receive 12 cycles of venetoclax-obinutuzumab (VenG) or chlorambucil-obinutuzumab (ClbG), impaired renal function was reported for most pts at study entry. However, TLS was a very rare finding in CLL14; here, we analyze the efficacy of measures implemented to prevent TLS and preliminary stages of TLS.
Methods
The CLL14 protocol specified categorization of pts according to their risk for TLS based on lymph node size (via CT/MRI) and lymphocyte count. Obinutuzumab was administered three times in the first cycle with recommended dose splitting at first administration; venetoclax was added on cycle 1 day 22 with a dose of 20 mg. A five-week ramp-up dosing to the target dose of 400mg daily was used to mitigate TLS risk. Monitoring and preventative measures were implemented according to each patient's TLS risk and included medication with uric acid reducers, fluid intake and laboratory assessments. Additionally, patients with high TLS risk were hospitalized with intensified laboratory monitoring, intravenous hydration and prophylactic use of rasburicase. TLS events were defined as per Howard criteria. Adverse events (AEs) were graded using the NCI Common Toxicity Terminology Criteria for Adverse Events v4.0.
Results
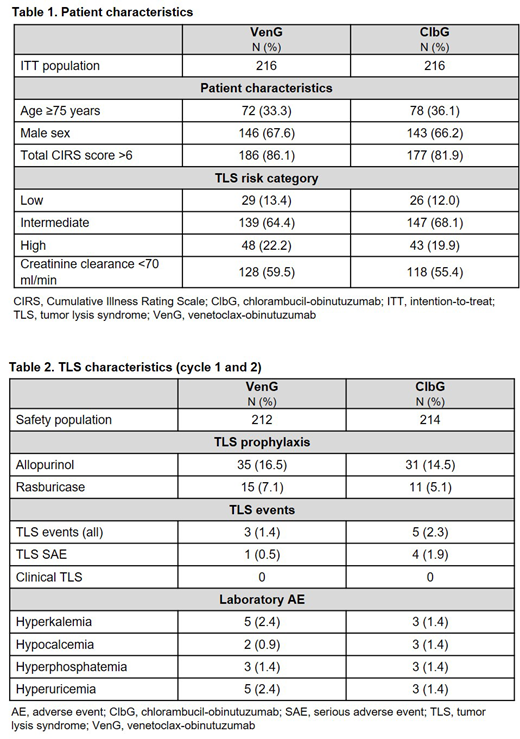
432 pts were randomized to either receive VenG (n=216) or ClbG (n=216). For VenG, TLS risk was categorized as low in 29 pts (13.4%), medium in 139 pts (64.4%) and high in 48 pts (22.2%). For ClbG, TLS risk was assessed as low in 26 (12.0%), medium in 147 (68.1%) and high in 43 (19.9%) pts. Median creatinine clearance was 65.2 ml/min in the VenG and 67.52 ml/min in the ClbG arm; overall, 57.5% of pts had a clearance below 70 ml/min.
TLS occurred in 3 pts (0.5%) in the VenG arm and 5 pts (2.3%) in the ClbG arm. No clinical TLS was observed. All pts were hospitalized or hospitalization was prolonged due to TLS. All TLS events in the VenG arm occurred prior to the first dose of venetoclax and were associated with obinutuzumab; 1 pt was assessed as low-risk and 2 as medium-risk for TLS. All pts had received prophylaxis with allopurinol prior to treatment start. In all cases, TLS occurred on cycle 1 day 2 after the first infusion of obinutuzumab.
For ClbG, TLS occurred in 1 pt with low risk, 3 with medium risk and 1 with high risk of TLS. All events occurred on cycle 1 day 1 or day 2. All but 2 pts received allopurinol prophylaxis.
Apart from these AEs, 12 pts in the VenG arm experienced lab abnormalities consistent with Howard criteria during cycle 1 and 2. All but 2 pts had TLS prophylaxis documented. Six of these had medium and 6 had high risk of TLS. In 5 pts, lab abnormalities occurred after obinutuzumab and prior to venetoclax dosing. In 4 pts, 1 of the 2 lab values was already abnormal prior to Ven dosing (elevated uric acid in 3 pts and elevated phosphate in 1 pt). In 1 pt, lab abnormalities meeting Howard criteria were observed pre-dose. In 2 pts, lab abnormalities were observed post-dose. All of these abnormalities were assessed by the investigator as not-clinically significant, apart from 3 AEs of single electrolyte abnormalities (Table 1). No treatment was administered and no modifications to venetoclax dosing were performed due these laboratory abnormalities.
For ClbG, 6 pts experienced lab abnormalities. One pt was assessed as low, 3 as medium and 2 as high risk for TLS. All pts received TLS prophylaxis. All abnormal values occurred after obinutuzumab infusion. Two AEs of single electrolyte abnormalities were reported (Table 1). One pt received rasburicase for treatment of hyperuricemia, otherwise no treatments were administered.
Conclusion
This report shows that, in the CLL14 protocol, treatment with VenG could be managed in a way that allowed control of TLS. Of high clinical relevance, not a single clinical or life-threatening TLS event was observed with venetoclax, indicating the measures used in the protocol were effective in preventing this condition, even in a population of elderly patients with relevant comorbidity including chronic kidney disease.
Al-Sawaf:Roche: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: travel support; Janssen: Membership on an entity's Board of Directors or advisory committees, Other: travel support; AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: travel support; Gilead: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: travel support. Fink:Janssen: Membership on an entity's Board of Directors or advisory committees; Roche: Other: Travel grants; Celgene: Research Funding. Sinha:Roche Products Ltd: Employment. Tandon:Roche Products Ltd: Employment; Roche: Equity Ownership. Eichhorst:Gilead Sciences, Inc.: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Roche: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Novartis: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Celgene: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; AbbVie: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; ArQule: Membership on an entity's Board of Directors or advisory committees; BeiGene: Research Funding. Fischer:AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees; Roche: Other: travel grants. Hallek:Roche: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Gilead: Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Janssen: Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Celgene: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Boehringer Ingelheim: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal