

Introduction: Ibrutinib, an irreversible inhibitor of Bruton's tyrosine kinase, is an established therapeutic agent in a variety of B-cell lymphoproliferative disorders. Ibrutinib induces platelet dysfunction and concurrent treatment with ibrutinib and warfarin was shown to significantly increase the risk of bleeding. The current study was designed to investigate the safety of direct oral anticoagulants (DOACs) in patients receiving ibrutinib, considering their expanding employment together with the lack of data regarding their safety in patients receiving ibrutinib.
Methods: We conducted a retrospective cohort study to evaluate risks of major bleeding in patients with B-cell lymphoproliferative disorders (CLL, MCL, DLBCL, MZL or WM) that were treated with ibrutinib and DOACs but without concurrent antiplatelet therapy, between January 2010 and October 2018 in 5 participating centers. Patient medical charts were reviewed for demographic parameters, comorbidities, ibrutinib dosage, DOACs dosage (including the adjustment for renal function), blood count and chemistry tests, bleeding site and grade.
Results: The study included 30 patients, median age at starting concurrent administration of ibrutinib and DOACs was 71.58 years (range 50.9-88.2). Most patients were treated for CLL (n=18, 60%) and MCL (n=8, 26%). The most common daily doses of ibrutinib were 420 mg and 560 mg in 63.3% and 30% of patients respectively. None of the patients received an additional antiplatelet agent. Twenty-three patients were treated with apixaban (76.7%), 4 with rivaroxaban (13.3%) and 3 (10%) with dabigatran. The main indications for DOACs were atrial fibrillation and VTE (venous thromboembolism).
The median follow-up after initiation of the ibrutinib-DOAC combination was 13.4 months (range 1.8-47.9 months). Bleeding was reported in 22 patients (73.3%), mostly mucocutaneous (n=12, 40%) and gastrointestinal tract (n=7, 23.3%), followed by CNS bleeding (n=4, 13.3%). Mucocutaneous bleedings were all grade 1-2 and gastrointestinal tract and CNS bleeding events were grade 1-4. Major bleeding events, defined as grade 3 or 4, occurred in 5 patients (16.6%) and did not result in death of any of the patients.
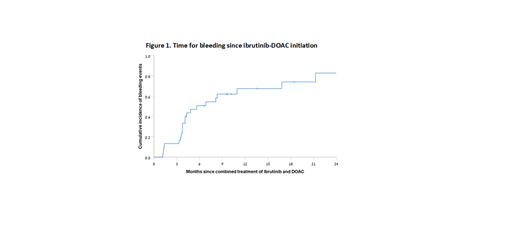
The median time for bleeding following ibrutinib-DOAC initiation was 5.6 months. Over a follow-up period of 21 months of combined treatment, the incidence of bleeding events (of all grades) increased to 75% (Figure 1). Incidence of bleeding events (including all grades) was quite similar between all DOAC subtypes (73.9% with apixaban, 75% with rivaroxaban and 66.7% with dabigatran). No statistically significant predictors for increased risk of bleeding in patients receiving ibrutinib combined with DOACs were detected.
Ibrutinib was stopped in 8 patients (26.7%) due to grade 1 to 4 bleeding events and was re-initiated in 6 patients, resulting in recurrent grade 3 and 4 bleeding events in 2 patients.
Conclusions: Concurrent administration of DOACs and ibrutinib appears to be feasible. However, risk of bleeding is not neglectable, and treatment resumption in patients that experienced a significant bleeding event should be considered with caution.
Arnason:Celgene/Juno: Consultancy; Regeneron Pharmaceuticals, Inc.: Consultancy. Herishanu:Roche: Honoraria; AbbVie: Honoraria; Janssen: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal