

Prior studies have evaluated incidence and survival trends for B-Acute Lymphoblastic Leukemia (B-ALL) in children and adults. However, there have been no recent studies evaluating the difference in survival between different race and ethnicities in the era of tyrosine kinase inhibitors and novel combination therapy. We wanted to determine 5-year observed survival for adult patients with B-ALL diagnosed in recent years and assess for any difference in survival by race-ethnicity.
Methods:
We used Surveillance Epidemiology End Results (SEER) 18 registry to identify B-ALL patients using ICD-O-3 codes 9811-9818 and 9836. SEER 18 covers ~28% of US population. The year of diagnosis was limited to 2010-2016 in order to capture a patient population most likely treated with modern therapies. We limited our study to adults aged 20 years (yrs) or more, which were then divided into the following age groups: 20-29, 30-39, 40-49, 50-59, 60-69,70-79,80+ yrs of age. Gender, race-ethnicity, median family income and observed overall survival (OS) were obtained from SEER. For multivariate survival analysis, Cox proportional hazard model was used to adjust for clinically important and other relevant variables (age, gender, race-ethnicity, median income). We included median family income, a county level characteristic in our analysis as a surrogate for access to care. We divided these counties into quintiles based on median family income and included that variable in the multivariate model. We did not adjust for genetic risk or patient insurance status, as the information provided in SEER was inadequate and would likely lead to misclassification bias. SEER Stat 8.3.5 and SAS student edition were used for analysis.
Results:
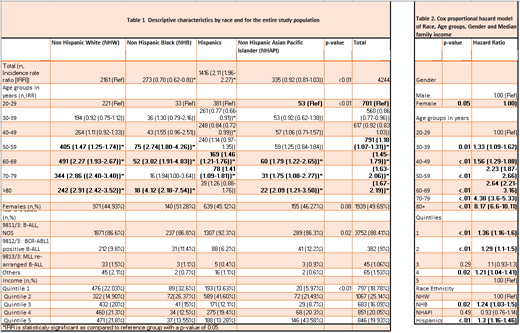
4244 cases of B-ALL were identified with an age adjusted incidence rate of 0.92 per 100,000. B-ALL occurred at all ages, but incidence was higher in young adults (<30 yrs) and adults older than 50 yrs of age, with peak incidence noted in the oldest age group (80+yrs). Of note, our cohort included adults older than or equal to 20 yrs of age, hence did not capture the early peak of childhood B-ALL. Females had a statistically significant lower incidence of B-ALL as compared to males (Incidence rate ratio (IRR) 0.77, p-value<0.05). Table 1 lists counts and IRR by different patient characteristics.
Age adjusted incidence was the highest among Hispanics (1.61{1.53-1.71}), followed by Non-Hispanic Whites (NHW)(0.77{0.73-0.8}, Non-Hispanic Asian Pacific Islander (NHAPI)(0.7{0.63-0.78}) and Non-Hispanic Blacks (NHB)(0.54{0.47-0.61}); this difference was statistically significant (p-value <0.05). When we evaluated the age adjusted incidence rate in each age group by different race-ethnicities, Hispanics had a statistically significant higher incidence in each age group except in 80+ yrs age group.
About 52% of population died during the study period from any cause. We limited our survival analysis to patients without second malignancy to avoid the confounding effect of another cancer associated mortality. We evaluated OS differences between race-ethnicity in a multivariate model that adjusted for age, sex and income. We found that when compared to NHW, Hispanics (Hazard Ratio (HR) 1.3{1.16-1.46}; p<0.01) and NHB (HR 1.24{1.03-1.5};p 0.02) had worse overall survival. We also showed increased mortality in older than younger adults with B-ALL (Table 2), in line with prior knowledge. There was slightly decreased OS seen in males compared to females, and the difference barely reached statistical significance (HR 0.91{0.83-1.0}; p 0.05). Patients from the poorest counties had worse survival than those in counties with higher median income (Table 2).
Conclusion:
Our study showed a significant survival disparity in adult B-ALL by race and ethnicity in the modern era. This can partly be attributed to differences in access to care as shown in our study. Interestingly, Hispanic and NHB have a significantly worse overall survival compared to NHW and NHAPI even after accounting for income differences, as a surrogate for access to care. This could be due to other unaccounted measure of health disparity, availability of allogeneic transplantation and/or difference in disease biology. Further studies are needed to evaluate such differences, identify barriers to care in minority populations and characterize potential differences in the genetic make-up of B-ALL in the various ethnic/racial groups.
Sica:Physician's Education Resources (PER): Honoraria. Verma:Stelexis: Equity Ownership, Honoraria; Acceleron: Honoraria; Celgene: Honoraria; BMS: Research Funding; Janssen: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal