

Introduction: Lower-risk MDS is characterized by anemia and ineffective erythropoiesis leading to RBC transfusion dependence. Effective treatment for anemia remains an unmet medical need. Patients with MDS may also experience additional cytopenias that may complicate treatment and contribute to infections and bleeding events.
Here, we report hematologic improvement (HI) outcomes for patients in the MEDALIST trial (ClinicalTrials.gov identifier: NCT02631070), a phase 3, randomized, double-blind, placebo-controlled study evaluating the efficacy and safety of luspatercept, a first-in-class erythroid maturation agent that binds select TGF-β superfamily ligands to reduce aberrant Smad2/3 signaling and enhance late-stage erythropoiesis.
Methods: Eligible patients in the MEDALIST trial were adults with anemia due to Very low-, Low-, or Intermediate-risk MDS with RS according to the Revised International Prognostic Scoring System; were refractory, intolerant, or ineligible to receive erythropoiesis-stimulating agents (ESAs); and required RBC transfusions. Patients received luspatercept (starting dose of 1.0 mg/kg and titration up to 1.75 mg/kg, if needed) or placebo subcutaneously every 3 weeks for ≥ 24 weeks. Platelet and neutrophil counts were assessed by the central laboratory. Secondary endpoints included HI-neutrophil (HI-N) and -platelet (HI-P) responses, using International Working Group 2006 criteria, over any consecutive 56-day period. Mean changes from baseline in platelets and neutrophils were also evaluated.
Results*: A total of 94.8% patients in the luspatercept arm and 97.4% in the placebo arm had refractory cytopenia with multilineage dysplasia and RS at baseline. Mean neutrophil and platelet counts at baseline for patients in the luspatercept arm were 2.8 x 109/L and 259 x 109/L, respectively, and in the placebo arm were 2.7 x 109/L and 252 x 109/L, respectively. Neutropenia (< 1 x 109/L) was confirmed at baseline in 15 (9.8%) and 10 (13.2%) patients in the luspatercept and placebo arms, respectively. Fifty-one (33.3%) patients in the luspatercept arm and 22 (28.9%) in the placebo arm received granulocyte colony-stimulating factor in combination with ESAs prior to randomization. A total of 8 (5.2%) and 6 (7.9%) patients receiving luspatercept and placebo, respectively, had baseline thrombocytopenia (< 100 x 109/L); no patients received prior platelet transfusions.
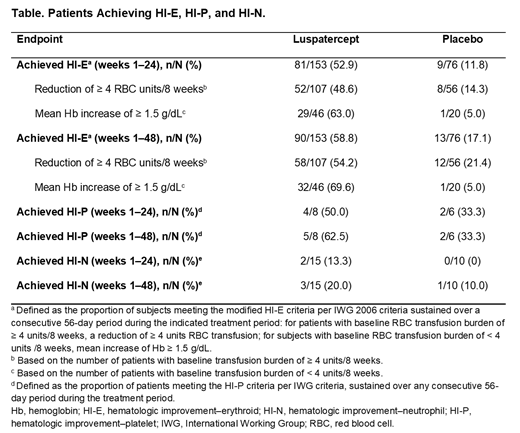
Fifteen (9.8%) and 10 (13.2%) patients in the luspatercept and placebo arms, respectively, were evaluable for HI-N (i.e. baseline neutrophils < 1 x 109/L); 3/15 (20%) of those receiving luspatercept and 1/10 (10%) of those receiving placebo achieved HI-N in Weeks 1-48. Among patients who were evaluable for HI-P (i.e. baseline platelets < 100 x 109/L), 5/8 (62.5%) of those receiving luspatercept and 2/6 (33%) of those receiving placebo achieved HI-P in Weeks 1-48 (Table). None of the luspatercept HI-P responders received platelet transfusions.
Mean changes from baseline in neutrophils of 0.94 x 109/L with luspatercept and 0.04 x 109/L with placebo were observed at Week 15, with early increases reported for luspatercept by Day 8 (0.86 vs 0.08 x 109/L for placebo). Mean increases in neutrophils at Day 8 occurred in both luspatercept responders (by MEDALIST primary endpoint; 1.0 x 109/L) and non-responders (0.8 x 109/L). Mean changes from baseline in platelets of 29 x 109/L were observed with luspatercept and 0.9 x 109/L with placebo by Week 12, but early increases were observed with luspatercept by Day 8 (18 vs 3 x 109/L for placebo) and mean increases in platelets at Day 8 occurred in both luspatercept responders (21.4 x 109/L) and non-responders (16.5 x 109/L).
No patients in either arm experienced grade 3 or 4 treatment-emergent thrombocytopenia. Treatment-related grade 3 or 4 neutropenia was reported in 1 (0.7%) patient receiving luspatercept and 1 (1.3%) patient receiving placebo.
Conclusions: Although only a minority of patients were evaluable for HI-P/HI-N response based on entry criteria for the study, luspatercept treatment resulted in a mean increase from baseline in platelet and neutrophil counts in most patients overall vs placebo, regardless of response status. These improvements were observed early following treatment initiation and then stabilized. Luspatercept did not contribute to the worsening of cytopenias vs placebo.
*Data cutoff: May 8, 2018.
Garcia-Manero:Amphivena: Consultancy, Research Funding; Helsinn: Research Funding; Novartis: Research Funding; AbbVie: Research Funding; Celgene: Consultancy, Research Funding; Astex: Consultancy, Research Funding; Onconova: Research Funding; H3 Biomedicine: Research Funding; Merck: Research Funding. Mufti:Celgene Corporation: Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Cellectis: Membership on an entity's Board of Directors or advisory committees, Research Funding. Fenaux:Celgene Corporation: Honoraria, Research Funding; Astex: Honoraria, Research Funding; Jazz: Honoraria, Research Funding; Aprea: Research Funding. Buckstein:Takeda: Research Funding; Celgene: Consultancy, Honoraria, Research Funding. Santini:Acceleron: Membership on an entity's Board of Directors or advisory committees; Amgen: Membership on an entity's Board of Directors or advisory committees; Menarini: Membership on an entity's Board of Directors or advisory committees; Celgene Corporation: Honoraria, Membership on an entity's Board of Directors or advisory committees; Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees; Johnson & Johnson: Honoraria. Díez-Campelo:Celgene Corporation: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Novartis: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding. Finelli:Celgene Corporation: Consultancy, Research Funding, Speakers Bureau; Novartis: Consultancy, Speakers Bureau; Janssen: Consultancy, Speakers Bureau. Sekeres:Syros: Membership on an entity's Board of Directors or advisory committees; Millenium: Membership on an entity's Board of Directors or advisory committees; Celgene: Membership on an entity's Board of Directors or advisory committees. List:Celgene: Membership on an entity's Board of Directors or advisory committees, Research Funding. Laadem:Celgene Corporation: Employment, Equity Ownership. Ito:Celgene Corporation: Employment, Equity Ownership. Zhang:Celgene Corporation: Employment, Equity Ownership. Rampersad:Celgene Corp: Employment, Equity Ownership. Sinsimer:Celgene Corporation: Employment, Equity Ownership. Linde:Fibrogen, Inc.: Equity Ownership; Abbott Laboratories, Inc.: Equity Ownership; Acceleron Pharma: Employment, Equity Ownership. Platzbecker:Celgene: Consultancy, Honoraria; Novartis: Consultancy, Honoraria; Abbvie: Consultancy, Honoraria. Komrokji:Alexion: Speakers Bureau; Incyte: Consultancy; Janssen: Consultancy; Agios: Consultancy; Celgene: Consultancy; Pfizer: Consultancy; Jazz: Speakers Bureau; DSI: Consultancy; Novartis: Speakers Bureau.
Luspatercept is an investigational therapy that is not approved for any use in any country. Luspatercept is currently being evaluated for potential use in patients with anemia due to myelodysplastic syndromes, beta-thalassemia, or myelofibrosis.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal