

Background: Patients (pts) with myelofibrosis (MF) suffer from a wide range of possibly debilitating disease manifestations (e.g. splenomegaly, weight loss, fatigue, night sweats, pain etc) resulting in severe symptom burden and quality of life decrement. Compared to INT-2/HIGH IPSS risk categories, lower risk pts display a less severe disease burden at diagnosis; nonetheless, with no active therapy, disease severity increases over time in all risk categories (Mesa et al, Leuk Res 2013). ROMEI (CINC424AIT04-Ruxolitinib Observational study in Myelofibrosis treated patiEnts in Italy) is a prospective observational study focused on real-life management of MF pts treated with ruxolitinib (RUX). The prospective assessment of the Myeloproliferative Neoplasm 10 (MPN 10) total score over time and the EQ-5D-5L and its related general health EQ-VAS values over time were included as primary endpoints and changes in spleen length were instead included as secondary endpoint.
Aims: To analyze the extent lower-risk MF pts treated with RUX may differentiate from higher-risk pts treated with RUX in terms of disease characteristics at treatment start, toxicity and response. A sub-analysis of the ROMEI trial was performed to evaluate differences in disease burden (i.e symptoms according to MPN-10, general health status according to EQ-VAS and spleen length) at RUX start and its modification after 24 weeks (wks) of treatment between pts with different BL IPSS category.
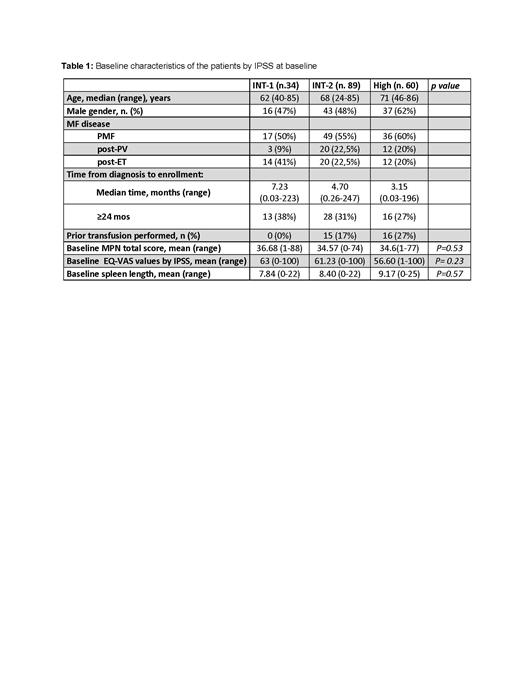
Methods: Out of 215 enrolled pts, 183 (96 male) were evaluable for this sub-analysis: 34 INT-1, 89 INT-2 and 60 HIGH risk pts based on IPSS. BL (BL) pts characteristics are shown in table 1. Pts started RUX according to Summary of Product Characteristics; MPN-10 scores and EQ-VAS values were collected at BL and at wks 4, 8, 12 and 24 after treatment start; spleen length by manual palpation was assessed at the same time points. Differences in IPSS subgroups were compared by means of analysis of variance (ANOVA) applied on rank transformed data in case of non-normal distribution. The BL value was included in the models on scoring changes.
Results:
MPN-10. In the overall cohort, we observed an improvement of MPN-10 score upon RUX start from 34.86±17.90 (range 0-88) at BL to 21.55±15.25 (range 0-70) at wk 24. No statistically differences were observed on MPN-10 total score between IPSS risk categories both at BL (P=0.83) and at wk 24 (P=0.53). Furthermore, the improvement in pts' symptoms evaluated by means of change of MPN-10 total score between wk 24 and BL resulted similar between the different IPSS risk categories (P=0.87).
EQ-VAS. In the overall group, EQ VAS values increased in mean from 59.88±20.23 (min; max: 0; 100) at BL to 67.36±18.57 (min; max: 10; 100) at wk 24. No differences between IPSS risk category were observed at BL (P=0.23, table 1).After 24 wks, EQ VAS was, in mean, 73.70±16.74 in INT-1 risk, 67.78±18.59 in INT-2 risk and 62.45±18.93 in HIGH risk with statistically differences between IPSS risk category (P=0.02) and, in particular, between HIGH and INT-1 risk (P=0.02). Difference between IPSS risk category was observed also when considering the change of EQ VAS between wk 24 and BL (P=0.02): the improvement in pts' health status resulted statistically lower in pts with HIGH compared to INT-1 (P=0.01) while no difference between INT-2 and INT-1 risk was observed (P=0.07).
Spleen length. Among evaluable pts, spleen length at BL seemed to increase as the IPSS risk category increased: 7.84±5.64 cm in INT-1 risk, 8.40±5.08 cm in INT-2 risk and 9.17±6.24 cm in HIGH, but no statistical difference was found between the groups (P=0.57). At week 24 mean spleen length decreased in all subgroups: 4,53±5.99 cm in INT-1 risk, 3.90±4.29 cm in INT-2 risk and 5.39±6.52 cm in HIGH risk but again with no statistical difference between groups (P= 0.77). Furthermore, the change of palpable spleen length between wk 24 and BL resulted similar between IPSS risk categories (P=0.55).
Conclusion: Our sub analysis suggests that disease burden can be very disabling even in INT-1 pts and comparably as in higher-risk categories. We also demonstrate that the EQ-VAS questionnaire may detect and quantify a wide range of symptoms not adequately included in IPSS risk stratification. Despite improvements in symptoms and splenomegaly were comparable across age groups, general health status improvement was significantly better in INT-1 pts. Further analysis will be available at the meeting.
Palandri:Novartis: Consultancy, Honoraria. Breccia:Novartis: Honoraria; Pfizer: Honoraria; BMS: Honoraria; Celgene: Honoraria; Incyte: Honoraria. Palumbo:Teva: Honoraria; Novartis: Honoraria; Janssen: Honoraria; Celgene: Honoraria; Amgen: Honoraria; Hospira: Honoraria. Abruzzese:BMS: Consultancy; Incyte: Consultancy; Novartis: Consultancy; Pfizer: Consultancy. Liberati:AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Clinical trial support; Roche: Other: Clinical trial support; Amgen: Membership on an entity's Board of Directors or advisory committees, Other: Clinical trial support; Celgene: Honoraria, Other: Clinical trial support; Bristol-Myers Squibb: Honoraria; Takeda: Membership on an entity's Board of Directors or advisory committees; Incyte: Consultancy; Servier: Honoraria, Membership on an entity's Board of Directors or advisory committees; Novartis: Other: Clinical trial support; Janssen: Honoraria. Pane:Novartis: Membership on an entity's Board of Directors or advisory committees, Other: research founding; Janssen: Membership on an entity's Board of Directors or advisory committees; GSK: Membership on an entity's Board of Directors or advisory committees; Amgen: Membership on an entity's Board of Directors or advisory committees; BMS: Membership on an entity's Board of Directors or advisory committees. Tiribelli:Novartis: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Pfizer: Membership on an entity's Board of Directors or advisory committees; Incyte: Membership on an entity's Board of Directors or advisory committees. Foà:Celltrion: Membership on an entity's Board of Directors or advisory committees; Novartis: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Shire: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Roche: Consultancy, Speakers Bureau; Janssen: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Amgen Inc.: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Pfizer: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Incyte: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Amgen Inc.: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Celltrion: Membership on an entity's Board of Directors or advisory committees; Janssen: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Novartis: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Incyte: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Roche: Consultancy, Speakers Bureau; Pfizer: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Shire: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Abbvie: Consultancy, Speakers Bureau; Abbvie: Consultancy, Speakers Bureau. Elli:Novartis: Membership on an entity's Board of Directors or advisory committees. Caocci:Novartis: Honoraria; Celgene: Honoraria. Morelli:Novartis: Employment. Passamonti:Janssen: Consultancy, Speakers Bureau; Novartis: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Roche: Consultancy, Speakers Bureau; Celgene Corporation: Consultancy, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal