

Background
Follicular lymphoma (FL) remains an incurable disease characterized by a persistent risk of relapse and progression. Therefore, to effectively delay progression of disease while maintaining patient quality of life, it is critical that clinicians select therapy for patients with newly diagnosed FL that most optimizes clinical outcomes. To help inform frontline treatment decisions among healthcare providers (HCPs) who care for patients with FL, we have developed an online treatment decision support tool that provides case-specific, individual recommendations from multiple experts. Here we present data from an analysis of self-reported practice trends from HCPs using the tool and compared with corresponding treatment recommendations from FL experts.
Methods
In May 2018, 5 experts in lymphoma patient care provided specific treatment recommendations for 72 distinct case scenarios of newly diagnosed FL defined by a simplified set of key patient and disease characteristics: disease stage, tumor grade, tumor bulk or burden, presence of symptoms, age and fitness, and patient's primary goal for treatment. Participating HCPs used selection menus to enter specific patient and disease factors along with their intended treatment plan for the case. After completing case entry, individual expert treatment recommendations for that specific patient case were displayed, followed by a short survey designed to determine the impact of the expert recommendations on the HCP's planned course of treatment.
Results
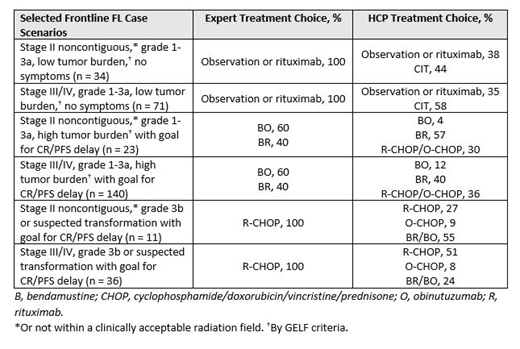
From August 2018 to July 2019, 311 HCPs (86% MDs) entered 522 patient case scenarios into the online tool. Among the 5 experts, there was a majority consensus in treatment selection for 89% of newly diagnosed FL cases. However, a comparison of expert and HCP treatment choices showed substantial variability for several different patient case scenarios (Table). For example, more than 40% of HCPs recommended chemoimmunotherapy (CIT) for patients with grade 1-3a FL with low tumor burden and no symptoms in contrast to 100% of experts who recommended observation or single-agent rituximab. For patients with grade 1-3a FL, high tumor burden, and a goal to achieve CR or delay PFS, regardless of symptoms, more than 50% of HCPs chose a bendamustine-based CIT regimen in agreement with the experts. However, approximately one third of HCPs chose a more aggressive CHOP-based CIT regimen. For treatment of grade 3b disease or suspected transformation with the intention to achieve CR or delay PFS, more than 25% of HCPs would select a bendamustine-based CIT regimen as compared with 100% of experts who chose R-CHOP. Among the HCPs whose intended treatment plan differed from the consensus expert recommendation, 60% indicated that they would change their initial choice of treatment after viewing the expert recommendations.
Conclusions
Analysis of case data from this online treatment decision tool suggests ongoing differences in practice between experts and HCPs for multiple case scenarios of newly diagnosed FL, including examples of potential overtreatment in patients with low tumor burden and undertreatment of patients with suspected transformation. Consensus expert recommendations in this online tool changed the intended treatment plan of many HCPs using it and, therefore, has the potential to optimize the care of patients newly diagnosed with FL. A detailed comparison of expert and HCP practice for different case scenarios will be presented.
Burke:Gilead: Consultancy; Roche/Genentech: Consultancy; Celgene: Consultancy. Flowers:Celgene: Consultancy, Research Funding; Optimum Rx: Consultancy; Millenium/Takeda: Research Funding; Acerta: Research Funding; Genentech, Inc./F. Hoffmann-La Roche Ltd: Consultancy, Research Funding; TG Therapeutics: Research Funding; National Cancer Institute: Research Funding; Burroughs Wellcome Fund: Research Funding; AbbVie: Consultancy, Research Funding; BeiGene: Consultancy, Research Funding; Eastern Cooperative Oncology Group: Research Funding; V Foundation: Research Funding; Denovo Biopharma: Consultancy; Gilead: Consultancy, Research Funding; Karyopharm: Consultancy; AstraZeneca: Consultancy; Pharmacyclics/Janssen: Consultancy, Research Funding; Spectrum: Consultancy; Bayer: Consultancy. Fowler:Celgene: Membership on an entity's Board of Directors or advisory committees, Research Funding; Roche: Membership on an entity's Board of Directors or advisory committees, Research Funding; ABBVIE: Membership on an entity's Board of Directors or advisory committees, Research Funding; TG Therapeutics: Membership on an entity's Board of Directors or advisory committees, Research Funding; Novartis Pharmaceuticals Corporation: Consultancy; Janssen: Membership on an entity's Board of Directors or advisory committees, Research Funding. Sharman:AbbVie: Consultancy, Honoraria, Research Funding; Janssen: Consultancy, Research Funding; Genentech: Consultancy, Honoraria, Research Funding; AstraZeneca: Consultancy, Honoraria, Research Funding; TG Therapeutics: Consultancy, Honoraria, Research Funding; Pharmacyclics LLC, an AbbVie Company: Consultancy, Honoraria, Research Funding; Acerta: Consultancy, Honoraria, Research Funding. Flinn:F. Hoffmann-La Roche Ltd: Research Funding; TG Therapeutics, Trillum Therapeutics, Abbvie, ArQule, BeiGene, Curis, FORMA Therapeutics, Forty Seven, Merck, Pfizer, Takeda, Teva, Verastem, Gilead Sciences, Astra Zeneca (AZ), Juno Therapeutics, UnumTherapeutics, MorphoSys, AG: Research Funding; Acerta Pharma, Agios, Calithera Biosciences, Celgene, Constellation Pharmaceuticals, Genentech, Gilead Sciences, Incyte, Infinity Pharmaceuticals, Janssen, Karyopharm Therapeutics, Kite Pharma, Novartis, Pharmacyclics, Portola Pharmaceuticals: Research Funding; AbbVie, Seattle Genetics, TG Therapeutics, Verastem: Consultancy; TG Therapeutics, Trillum Therapeutics, Abbvie, ArQule, BeiGene, Curis, FORMA Therapeutics, Forty Seven, Merck, Pfizer, Takeda, Teva, Verastem, Gilead Sciences, Astra Zeneca (AZ), Juno Therapeutics, UnumTherapeutics, MorphoSys, AG: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal