

Introduction:
Primary central nervous system lymphoma (PCNSL) is a rare and aggressive primary brain tumor confined to the brain, eyes, and cerebrospinal fluid. Over the past few decades, prognosis for PCNSL has significantly improved due to the standard use of high dose methotrexate (MTX) containing treatment regimens. However, it remains unclear if the number of MTX doses and the addition of rituximab has an impact on clinical outcomes. The recent HOVON 105/ALLG NHL 24 study questioned the role of rituximab in the first line setting when combined with a MTX based polychemotherapy using only 4 doses of MTX and 6 doses of rituximab. Over the last 30 years, standard of care at Memorial Sloan Kettering Cancer Center (MSKCC) has evolved, allowing the comparison of patients receiving different numbers of MTX doses and those treated with and without rituximab. The purpose of this study was to describe clinical outcomes based on standard of care treatment changes.
Methods:
This single-center retrospective IRB approved study at MSKCC included patients with immunocompetent PCNSL, age ≥18 years and diagnosed between 1/1983-11/2017. Patients were identified through a departmental database and electronic medical record. The primary objective was to describe overall survival (OS) based on common prognostic markers such as age, KPS, MSKCC prognostic score class (RPA I- III), use of rituximab, and number of methotrexate cycles. Overall survival was calculated from the date of diagnosis to death or last follow-up using Kaplan-Meier methodology. When examining effect of MTX on OS, OS was calculated from date of last MTX cycle until death or last follow-up. Univariable and multivariable analysis for prognostic factors were analyzed using Cox proportional hazards regression.
Results:
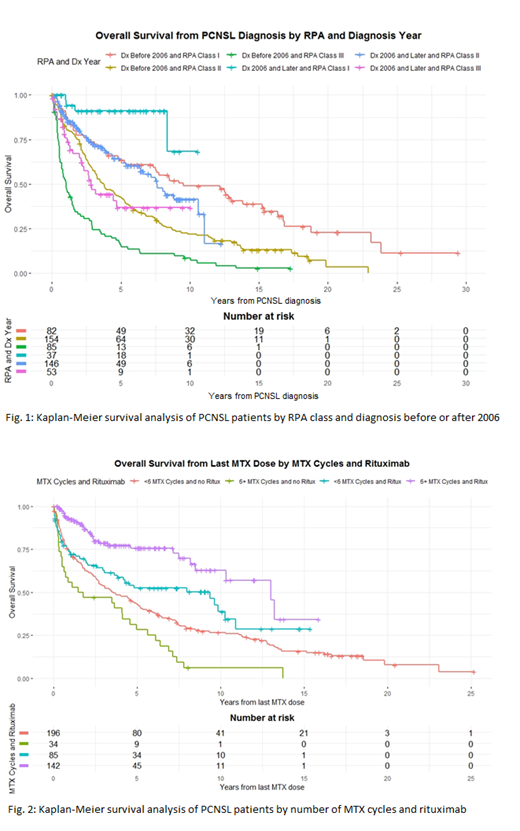
Five hundred and forty-six patients with newly diagnosed PCNSL were identified. Median age at diagnosis was 62 (range 19 to 90), median KPS was 70 (range 10 to 100), and 282 (52%) were men. In total, 472 patients (86.4%) received high dose MTX. Of 460 with known number of MTX cycles, 95 (20.7%) received 1-4 cycles and 365 (79.3%) received ≥5 cycles (5 cycles: 189, 41.1%, 6 cycles: 24, 5.2%, 7 cycles: 74, 16.1%, 8+ cycles: 78, 17%). Rituximab was given to 231 (42.3%). Three hundred and ten (56.8%) patients, treated before 2006, had been reported previously (historic cohort) and 236 (43.2%) served as contemporary cohort. Median OS of the entire population was 4.7 years (95% CI: 3.8-5.7); 3.3 years (95% CI: 2.8-4.1) in the historic and 8.1 years (95% CI: 6.6-no upper limit) in the contemporary cohort. Five-year OS was 40.3% (95% CI: 35.1-46.2) for the historical cohort and 61.8% (95% CI: 55.0-69.5) for the contemporary cohort. Median OS in the contemporary cohort improved in all RPA classes in comparison to patients treated before 2006 (RPA I: not yet reached vs 9.2 years; RPA II: 7.6 years vs 3.5 years; RPA III 2.8 years vs 1.0 year) (Fig. 1). For the historical cohort compared to the contemporary cohort, five-year OS changed from 62.8% to 91.0% in RPA I, 42.0% to 63.0% in RPA II, and 16.3% to 36.9% in RPA III. Patients receiving ≥ 6 cycles of MTX had a better clinical outcome (median OS from last MTX cycle: 7.8 years versus 4.3 years; HR 0.68 (95% CI (0.51 - 0.91), p=0.0085) on multivariable analysis adjusted for age, KPS, sex, RPA classes Additionally, the stratification of rituximab further elucidated the association between MTX cycles and OS, such that in patients receiving rituximab, those treated with ≥ 6 cycles of MTX experienced longer median OS compared to patients receiving < 6 cycles of MTX (13.0 years vs 9.4 years, p=0.001). Furthermore, in patients receiving ≥ 6 cycles of MTX, there was a survival benefit seen in patients who received rituximab compared to those who did not receive rituximab (13.02 years vs 1.61 years, p<000.1) (Fig.2).
Conclusions:
Overall survival for newly diagnosed PCNSL has improved significantly over the last few decades regardless of age, KPS, RPA class. Patients seem to benefit with the addition of rituximab and when receiving 6 or more cycles of MTX.
Grommes:BTG: Consultancy; Kite: Consultancy; Squipps: Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal