

Introduction: About 2 to 10% of patients (pts) diagnosed with Chronic Lymphocytic Leukemia (CLL) develop diffuse large B-cell lymphoma (DLBCL, so-called Richter transformation (RT)) over long-term follow-up. The outcomes of pts with RT are variable and poorly understood and there is no consensus on the best therapeutic approach. The aim of this study was to analyze the clinical characteristics, outcomes and factors predictive of survival in a large series of RT from the French Innovative Leukemia Organization (FILO).
Methods: Biopsy-confirmed RT (limited to DLBCL and excluding Hodgkin lymphoma) diagnosed from 2001 to 2018 were identified from eight FILO centers. Clinical and biological characteristics of CLL and RT at diagnosis, including cytogenetics, clonal relation with the pre-existing CLL, Epstein-Barr virus (EBV) status, cell of origin (COO) analyzed by immunohistochemistry and RT score (Tsimberidou AM et al, J Clin Oncol, 2006) were analyzed as well as treatment and outcomes. Overall survivals (OS) were defined as time from CLL and RT diagnosis to death from any cause and analyzed using the Kaplan-Meier method. Statistical analyses were performed with SAS version 9.4.
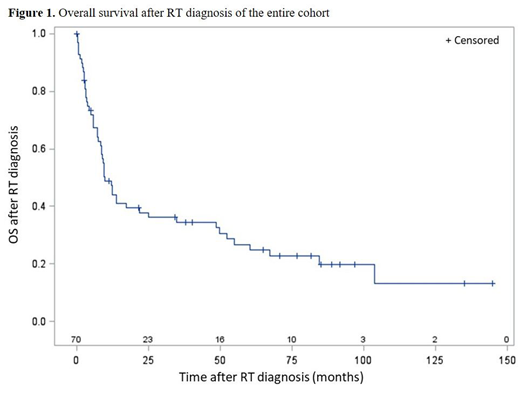
Results: A total of 70 CLL pts who developed RT were identified. The median age at CLL diagnosis was 62 years old (range 35-82), and 50 (71.4 %) were male. The median time to transformation was 5.5 years (range 0 to 22 years), with 12 simultaneous diagnosis of CLL and RT. Prior to RT, 20 (29%) pts had not been treated for CLL, 50 received one (n=21) or more (n= 29) line of treatment ; 6 pts had received a novel agent (ibrutinib, idelalisib or venetoclax). The median age at RT diagnosis was 68 years old (range 42-88). All biopsies were centrally reviewed; 38/58 pts (66%) had elevated LDH (>1.5N) ; 35/65 pts (54 %) had bulky disease (≥ 5 cm); 10/54 (18.5%) pts had del(17p) or TP53 mutation ; 9/42 pts (21%) had a complex karyotype (at least 3 abnormalities). The CLL and RT were clonally related in 27/27 (100%) tested pts. COO by Hans algorithm was non germinal center B cell-like (GCB) in 26/28 pts (93%). EBV was positive or detected in 5/40 (12.5%) pts. The median of Ki67 positivity was 70% (range 30% to 100%). The RT score (based at RT diagnosis on ECOG performance status 2-4, LDH >1.5 x normal, platelets<100 x 109/L, tumor size >5 cm and >1 prior therapy for CLL) was : low risk in 17 pts (31%), low-intermediate risk in 10 pts (19%), high-intermediate risk in 14 pts (25%) and high risk in 14 pts (25%). The most common first-line treatment of RT was immunochemotherapy (n=57, 87%) including R-CHOP-like regimen (n=48, 73%). Autologous or allogeneic transplantation was performed for 7 pts (11%). Response to first-line treatment was complete or partial response in 26 pts (40%), and stable disease or progression in 39 pts (60%). After a median follow-up of 8 years, 51/64 pts (80%) have died. The main causes of death were progressive DLBCL (n=36, 71%), infection (n=8, 16%) or progressive CLL (n=2, 4%). The median OS of the cohort from CLL and RT diagnosis (Figure 1) were 7.8 years and 9.5 months, respectively. In univariate analysis, patients with TP53 disruption at CLL stage, low platelets count, elevated LDH, elevated beta2-microglobulin, high ECOG score, high RT score, EBV positivity and absence of response to first-line RT treatment had worse OS. The ECOG score, platelets count and TP53 disruption remain significant in multivariate Cox-regression. Last, we compared the clinical and biological parameters of two Richter groups defined as: (i) short-term survivors (<12 months, n = 34) and (ii) long-term survivors (>48 months, n = 18). Long survival was significantly associated with elevated platelets count, low LDH, low ECOG, low RT score and response to RT first-line treatment.
Discussion: The clinical outcomes of RT patients is poor and novel treatment options are needed. However, a group of long-term survivors was identified, characterized by elevated platelets count, low LDH, low ECOG, low RT score and response to immunochemotherapy.
Leblond:Astra Zeneca: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Gilead: Honoraria, Speakers Bureau; Roche: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Abbvie: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Amgen: Honoraria, Speakers Bureau. Thieblemont:Roche: Honoraria, Research Funding; Gilead: Honoraria; Novartis: Honoraria; Kyte: Honoraria; Janssen: Honoraria; Celgene: Honoraria; Cellectis: Membership on an entity's Board of Directors or advisory committees. Cymbalista:Janssen: Honoraria; Gilead: Honoraria; AstraZeneca: Honoraria; Sunesis: Research Funding; Roche: Research Funding; Abbvie: Honoraria. Guièze:Abbvie: Honoraria; Janssen: Honoraria; Gilead: Honoraria; Roche: Honoraria. Broseus:Janssen: Honoraria; Gilead: Honoraria; Novartis: Research Funding. Feugier:gilead: Honoraria, Research Funding, Speakers Bureau; janssen: Honoraria, Research Funding, Speakers Bureau; abbvie: Honoraria, Research Funding, Speakers Bureau; roche: Honoraria, Research Funding, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal